Perpendicular serial maxillary distraction osteogenesis in cleft lip and palate patients
- PMID: 26981462
- PMCID: PMC4772552
- DOI: 10.4103/2231-0746.175778
Perpendicular serial maxillary distraction osteogenesis in cleft lip and palate patients
Abstract
Background: Cleft lip and palate patients often have a retruded maxilla with a severely narrowed deficient maxillary arch. This report aims to describe the management of severe maxillary retrusion and constriction in cleft lip and palate patients using distraction osteogenesis applied in serial sequence in two directions perpendicular to each other.
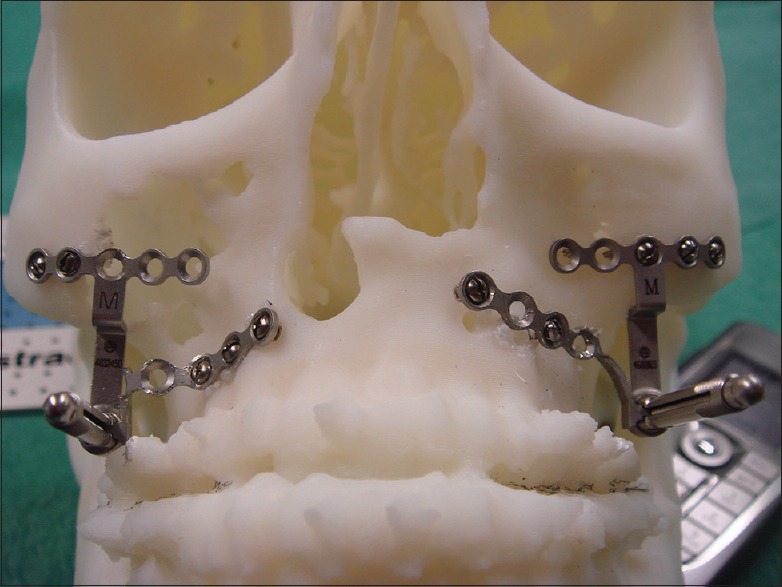
Materials and methods: Two adult male cleft lip and palate patients were treated with maxillary distraction osteogenesis in two stages. In the first stage, surgically assisted rapid palatal expansion with a tooth-borne device was performed to significantly expand the maxillary arch in the transverse dimension. After the teeth were orthodontically aligned, the horizontal distraction of the maxilla was made by two internal maxillary distraction devices.
Results: In the first patient, the maxilla was initially widened by 11 mm and then distracted forward by 20 mm. Despite the breakage of the shaft of one of the two distractors at the end of distraction, a satisfactory occlusion was found at the time of distractor device removal. The maxillary position has remained stable through 8 years of follow-up. In the second patient, the palate was widened by 14 mm and the maxilla was distracted forward by 22 mm. The maxillary position has remained stable through 3 years of follow-up.
Conclusion: Sequential serial distraction of maxilla in two planes perpendicular to each other is a safe and stable approach for the treatment of cleft lip and palate patients with severe transverse and anteroposterior discrepancies.
Keywords: Cleft lip and palate; maxillary distraction osteogenesis; palate expansion.
Figures


































References
-
- Harila V, Ylikontiola LP, Palola R, Sándor GK. Maxillary arch dimensions in cleft infants in Northern Finland. Acta Odontol Scand. 2013;71:930–6. - PubMed
-
- Harila V, Ylikontiola LP, Sándor GK. Dental arch relationships assessed by GOSLON Yardstick in children with clefts in Northern Finland. Eur J Paediatr Dent. 2014;15:389–91. - PubMed
-
- Molina F. Distraction osteogenesis for the cleft lip and palate patient. Clin Plast Surg. 2004;31:291–302. - PubMed
-
- Sándor GK, Ylikontiola LP, Serlo W, Pirttiniemi PM, Carmichael RP. Midfacial distraction osteogenesis. Atlas Oral Maxillofac Surg Clin North Am. 2008;16:249–72. - PubMed
-
- Balaji SM. History of craniofacial distraction osteogenesis. Abstracts of the Second Asia Pacific Congress on Distraction Osteogenesis. Bandos, Maldives. 2003:1–9.
LinkOut - more resources
Full Text Sources
Other Literature Sources