

Oral Phage Therapy of Acute Bacterial Diarrhea With Two Coliphage Preparations: A Randomized Trial in Children From Bangladesh
- PMID: 26981577
- PMCID: PMC4776075
- DOI: 10.1016/j.ebiom.2015.12.023
Oral Phage Therapy of Acute Bacterial Diarrhea With Two Coliphage Preparations: A Randomized Trial in Children From Bangladesh
Abstract
Background: Antibiotic resistance is rising in important bacterial pathogens. Phage therapy (PT), the use of bacterial viruses infecting the pathogen in a species-specific way, is a potential alternative.
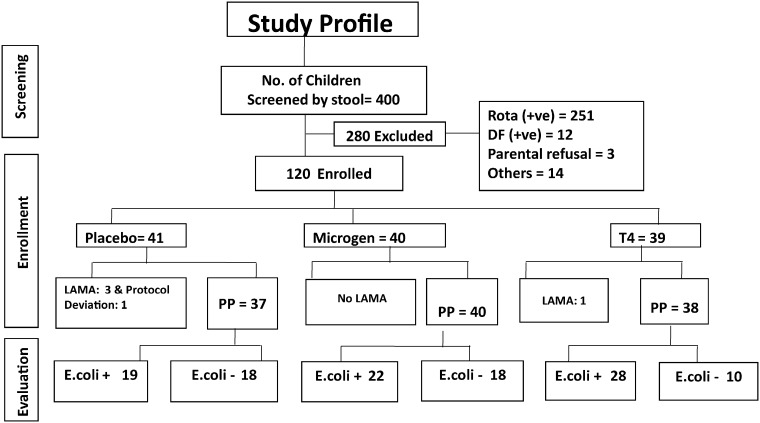
Method: T4-like coliphages or a commercial Russian coliphage product or placebo was orally given over 4 days to Bangladeshi children hospitalized with acute bacterial diarrhea. Safety of oral phage was assessed clinically and by functional tests; coliphage and Escherichia coli titers and enteropathogens were determined in stool and quantitative diarrhea parameters (stool output, stool frequency) were measured. Stool microbiota was studied by 16S rRNA gene sequencing; the genomes of four fecal Streptococcus isolates were sequenced.
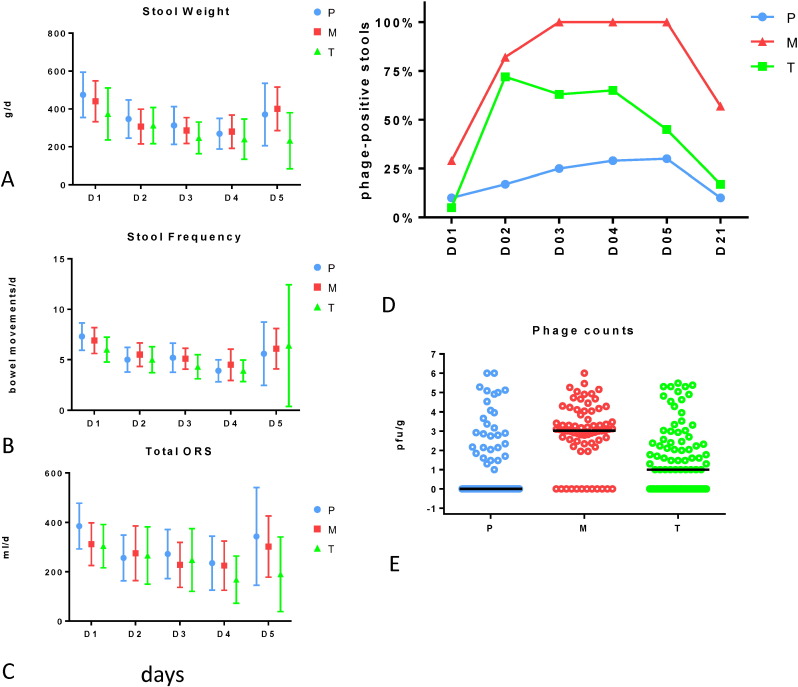
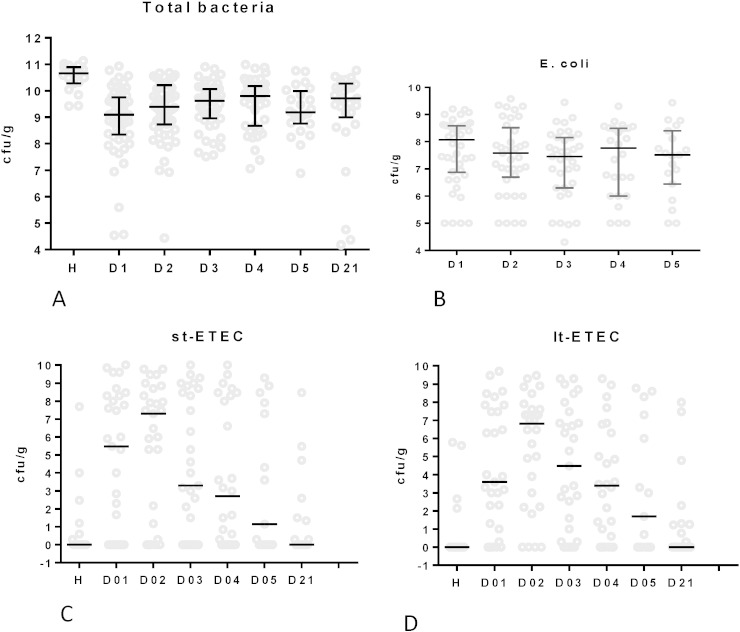
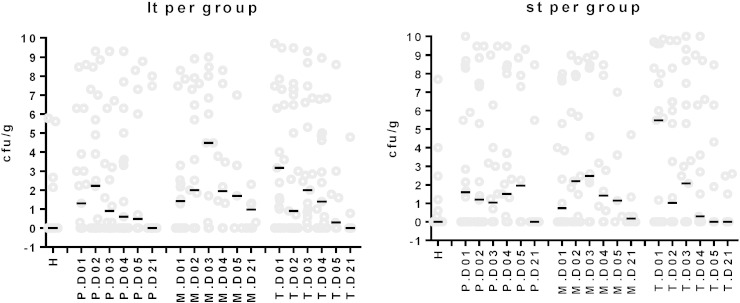
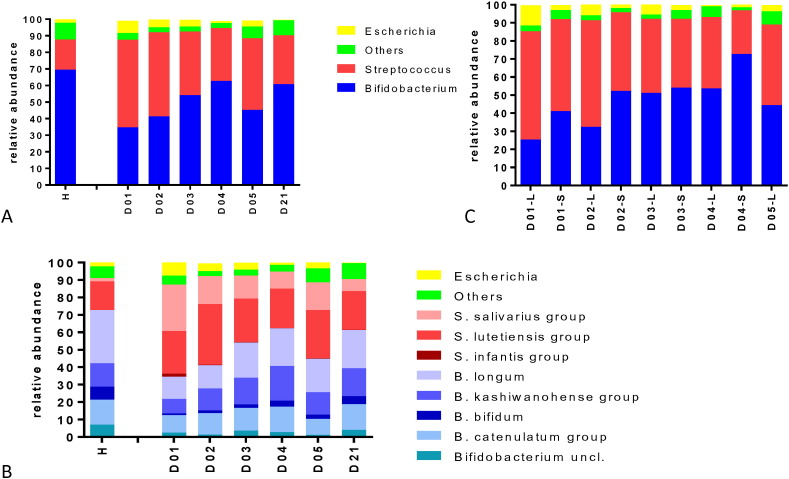
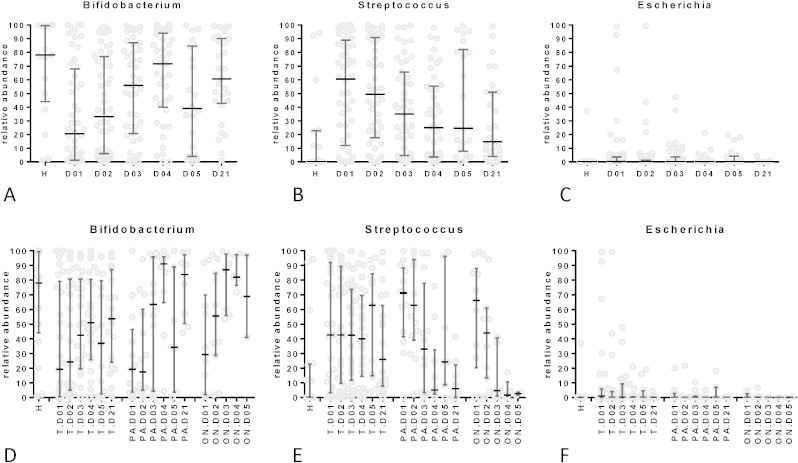
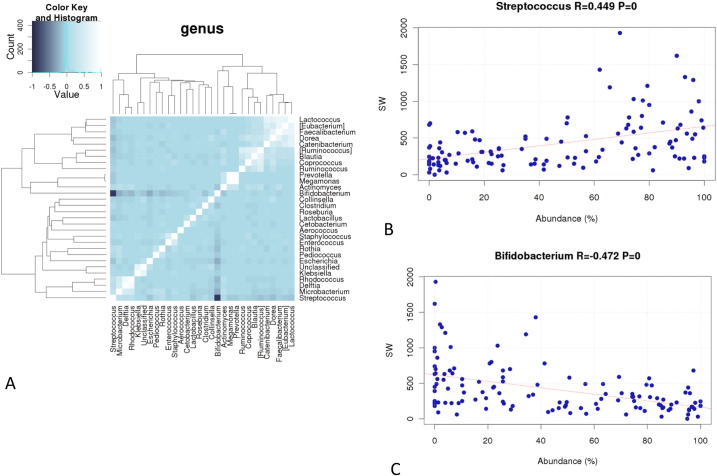
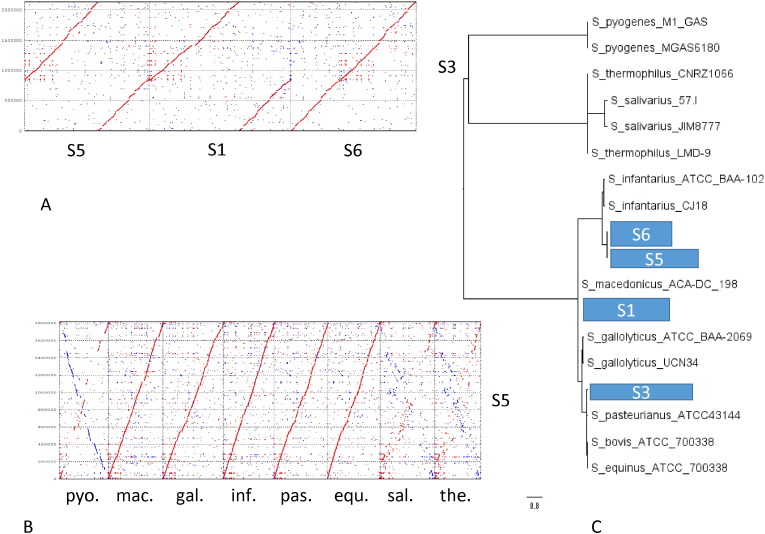
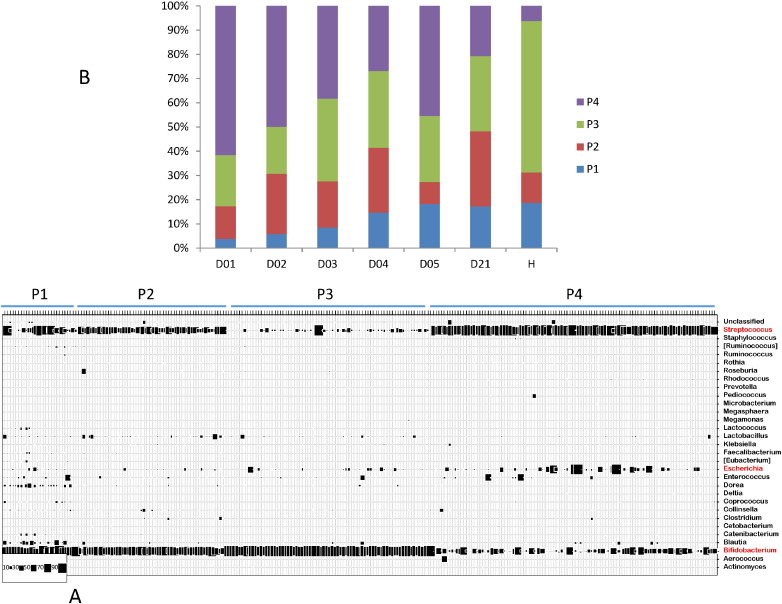
Findings: No adverse events attributable to oral phage application were observed (primary safety outcome). Fecal coliphage was increased in treated over control children, but the titers did not show substantial intestinal phage replication (secondary microbiology outcome). 60% of the children suffered from a microbiologically proven E. coli diarrhea; the most frequent diagnosis was ETEC infections. Bacterial co-pathogens were also detected. Half of the patients contained phage-susceptible E. coli colonies in the stool. E. coli represented less than 5% of fecal bacteria. Stool ETEC titers showed only a short-lived peak and were otherwise close to the replication threshold determined for T4 phage in vitro. An interim analysis after the enrollment of 120 patients showed no amelioration in quantitative diarrhea parameter by PT over standard care (tertiary clinical outcome). Stool microbiota was characterized by an overgrowth with Streptococcus belonging to the Streptococcus gallolyticus and Streptococcus salivarius species groups, their abundance correlated with quantitative diarrhea outcome, but genome sequencing did not identify virulence genes.
Interpretation: Oral coliphages showed a safe gut transit in children, but failed to achieve intestinal amplification and to improve diarrhea outcome, possibly due to insufficient phage coverage and too low E. coli pathogen titers requiring higher oral phage doses. More knowledge is needed on in vivo phage-bacterium interaction and the role of E. coli in childhood diarrhea for successful PT.
Funding: The study was supported by a grant from Nestlé Nutrition and Nestlé Health Science. The trial was registered with Identifier NCT00937274 at ClinicalTrials.gov.
Keywords: Bacteriophages; Bangladesh; Bifidobacterium; Cfu, colony forming unit; Children; Diarrhea; EAEC, enteroaggregative E. coli; EPEC, enteropathogenic E. coli; ETEC, enterotoxigenic E. coli; Escherichia coli; M, ColiProteus phage cocktail from Microgen; ORS, oral rehydration solution; P, placebo; PT, phage therapy; RCT, randomized controlled trial; Streptococcus; T, T4 phage cocktail from NRC; pfu, plaque forming unit; qPCR, quantitative polymerase chain reaction.
Figures
References
-
- Altschul S.F., Gish W., Miller W. Basic local alignment search tool. J. Mol. Biol. 1990;215:403–410. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
