

Long-term changes in dysnatremia incidence in the ICU: a shift from hyponatremia to hypernatremia
- PMID: 26983857
- PMCID: PMC4794471
- DOI: 10.1186/s13613-016-0124-x
Long-term changes in dysnatremia incidence in the ICU: a shift from hyponatremia to hypernatremia
Abstract
Background: Dysnatremia is associated with adverse outcome in critically ill patients. Changes in patients or treatment strategies may have affected the incidence of dysnatremia over time. We investigated long-term changes in the incidence of dysnatremia and analyzed its association with mortality.
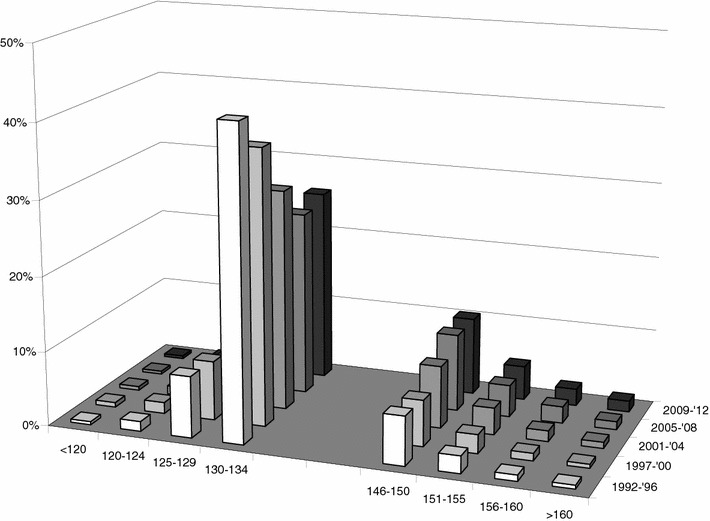
Methods: Over a 21-year period (1992-2012), all serum sodium measurements were analyzed retrospectively in two university hospital ICUs, up to day 28 of ICU admission for the presence of dysnatremia. The study period was divided into five periods. All serum sodium measurements were collected from the electronic databases of both ICUs. Serum sodium was measured at the clinical chemistry departments using standard methods. All sodium measurements were categorized in the following categories: <120, 120-124, 125-129, 130-134, 135-139, 140-145, 146-150, 151-155, 156-160, >160 mmol/L. Mortality was determined at 90 days after ICU admission.
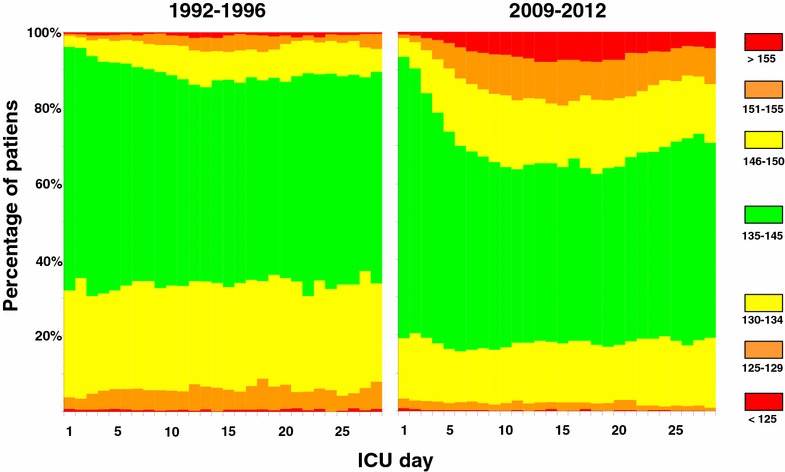
Results: In 80,571 ICU patients, 913,272 serum sodium measurements were analyzed. A striking shift in the pattern of ICU-acquired dysnatremias was observed: The incidence of hyponatremia almost halved (47-25 %, p < 0.001), whereas the incidence of hypernatremia nearly doubled (13-24 %, p < 0.001). Most hypernatremias developed after ICU admission, and the incidence of severe hypernatremia (sodium > 155 mmol/L) increased dramatically over the years. On ICU day 10 this incidence was 0.7 % in the 1992-1996 period, compared to 6.3 % in the 2009-2012 period (p < 0.001). More severe dysnatremia was associated with significantly higher mortality throughout the 21-year study period (p < 0.001).
Conclusions: In two large Dutch cohorts, we observed a marked shift in the incidence of dysnatremia from hyponatremia to hypernatremia over two decades. As hypernatremia was mostly ICU acquired, this strongly suggests changes in treatment as underlying causes. This shift may be related to the increased use of sodium-containing infusions, diuretics, and hydrocortisone. As ICU-acquired hypernatremia is largely iatrogenic, it should be-to an important extent-preventable, and its incidence may be considered as an indicator of quality of care. Strategies to prevent hypernatremia deserve more emphasis; therefore, we recommend that further study should be focused on interventions to prevent the occurrence of dysnatremias during ICU stay.
Keywords: Critical care; Dysnatremia; Hypernatremia; Hyponatremia; Incidence; Infusion; Sodium.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
