

0.9% saline is neither normal nor physiological
- PMID: 26984838
- PMCID: PMC4794509
- DOI: 10.1631/jzus.B1500201
0.9% saline is neither normal nor physiological
Abstract
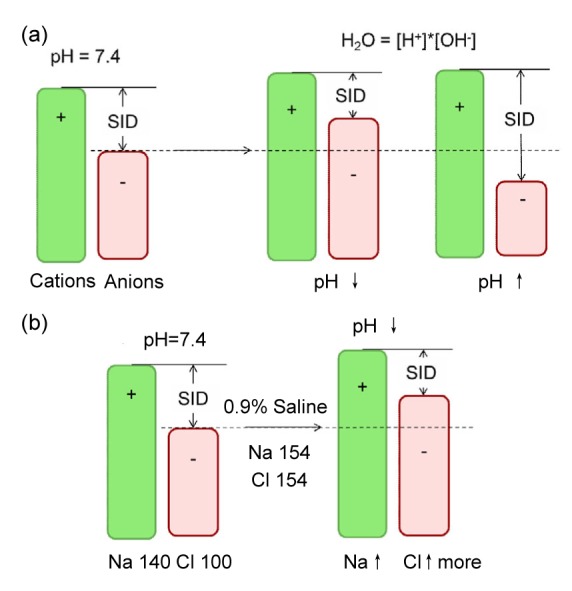
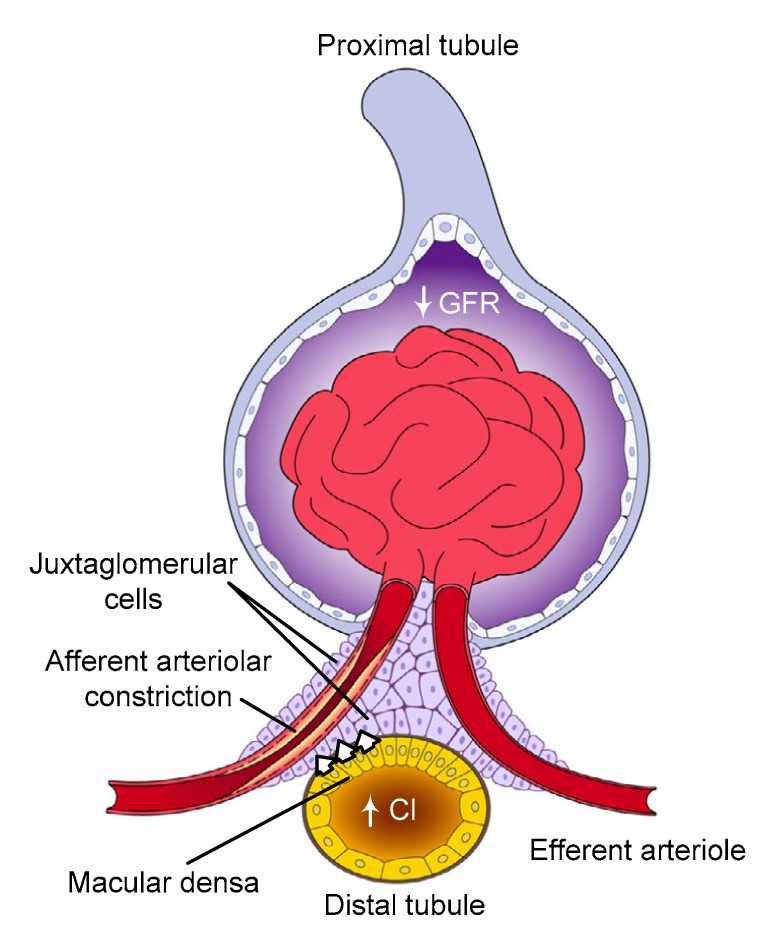
The purpose of this review is to objectively evaluate the biochemical and pathophysiological properties of 0.9% saline (henceforth: saline) and to discuss the impact of saline infusion, specifically on systemic acid-base balance and renal hemodynamics. Studies have shown that electrolyte balance, including effects of saline infusion on serum electrolytes, is often poorly understood among practicing physicians and inappropriate saline prescribing can cause increased morbidity and mortality. Large-volume (>2 L) saline infusion in healthy adults induces hyperchloremia which is associated with metabolic acidosis, hyperkalemia, and negative protein balance. Saline overload (80 ml/kg) in rodents can cause intestinal edema and contractile dysfunction associated with activation of sodium-proton exchanger (NHE) and decrease in myosin light chain phosphorylation. Saline infusion can also adversely affect renal hemodynamics. Microperfusion experiments and real-time imaging studies have demonstrated a reduction in renal perfusion and an expansion in kidney volume, compromising O2 delivery to the renal parenchyma following saline infusion. Clinically, saline infusion for patients post abdominal and cardiovascular surgery is associated with a greater number of adverse effects including more frequent blood product transfusion and bicarbonate therapy, reduced gastric blood flow, delayed recovery of gut function, impaired cardiac contractility in response to inotropes, prolonged hospital stay, and possibly increased mortality. In critically ill patients, saline infusion, compared to balanced fluid infusions, increases the occurrence of acute kidney injury. In summary, saline is a highly acidic fluid. With the exception of saline infusion for patients with hypochloremic metabolic alkalosis and volume depletion due to vomiting or upper gastrointestinal suction, indiscriminate use, especially for acutely ill patients, may cause unnecessary complications and should be avoided. More education regarding saline-related effects and adequate electrolyte management is needed.
Keywords: 0.9% saline; Acidosis; Balanced fluids; Hyperchloremia; Hyperkalemia; Renal hemodynamics.
Conflict of interest statement
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
Similar articles
-
Effects of saline infusion and acute metabolic acidosis and alkalosis on water and electrolyte transport in the human colon.Can J Physiol Pharmacol. 1977 Feb;55(1):13-20. doi: 10.1139/y77-003. Can J Physiol Pharmacol. 1977. PMID: 14780
-
Impact of normal saline infusion on postoperative metabolic acidosis.Paediatr Anaesth. 2009 Nov;19(11):1070-7. doi: 10.1111/j.1460-9592.2009.03126.x. Paediatr Anaesth. 2009. PMID: 19807885
-
The meaning of acid-base abnormalities in the intensive care unit: part III -- effects of fluid administration.Crit Care. 2005 Apr;9(2):204-11. doi: 10.1186/cc2946. Epub 2004 Sep 3. Crit Care. 2005. PMID: 15774079 Free PMC article. Review.
-
Effect of a single small volume fluid bolus with balanced or un-balanced fluids on chloride and acid-base status: a prospective randomized pilot study (the FLURES-trial).J Nephrol. 2024 Jun;37(5):1299-1308. doi: 10.1007/s40620-024-01912-z. Epub 2024 Mar 28. J Nephrol. 2024. PMID: 38546940 Clinical Trial.
-
Chloride toxicity in critically ill patients: What's the evidence?Anaesth Crit Care Pain Med. 2017 Apr;36(2):125-130. doi: 10.1016/j.accpm.2016.03.008. Epub 2016 Jul 28. Anaesth Crit Care Pain Med. 2017. PMID: 27476827 Review.
Cited by
-
Influence of normal saline on delayed graft function in kidney transplantation.Saudi J Anaesth. 2022 Oct-Dec;16(4):507-508. doi: 10.4103/sja.sja_167_22. Epub 2022 Sep 3. Saudi J Anaesth. 2022. PMID: 36337411 Free PMC article. No abstract available.
-
Hyperchloremia Is Associated With Poorer Outcome in Critically Ill Stroke Patients.Front Neurol. 2018 Jul 3;9:485. doi: 10.3389/fneur.2018.00485. eCollection 2018. Front Neurol. 2018. PMID: 30018587 Free PMC article.
-
Colorimetric detection of individual biothiols by tailor made reactions with silver nanoprisms.Sci Rep. 2021 Feb 16;11(1):3937. doi: 10.1038/s41598-021-83433-4. Sci Rep. 2021. PMID: 33594153 Free PMC article.
-
Antimicrobial Susceptibility Testing of Antimicrobial Peptides to Better Predict Efficacy.Front Cell Infect Microbiol. 2020 Jul 7;10:326. doi: 10.3389/fcimb.2020.00326. eCollection 2020. Front Cell Infect Microbiol. 2020. PMID: 32733816 Free PMC article. Review.
-
Dilutional acidosis during whole lung lavage under general anesthesia due to excessive absorption of normal saline.JA Clin Rep. 2022 Apr 14;8(1):30. doi: 10.1186/s40981-022-00520-9. JA Clin Rep. 2022. PMID: 35420327 Free PMC article.
References
-
- Awad S, Allison SP, Lobo DN. The history of 0.9% saline. Clin Nutr. 2008;27(2):179–188. (Available from: http://dx.doi.org/10.1016/j.clnu.2008.01.008) - DOI - PubMed
-
- Ballmer PE, McNurlan MA, Hulter HN, et al. Chronic metabolic acidosis decreases albumin synthesis and induces negative nitrogen balance in humans. J Clin Invest. 1995;95(1):39–45. (Available from: http://dx.doi.org/10.1172/JCI117668) - DOI - PMC - PubMed
-
- Barak M, Rudin M, Vofsi O, et al. Fluid administration during abdominal surgery influences on coagulation in the postoperative period. Curr Surg. 2004;61(5):459–462. (Available from: http://dx.doi.org/10.1016/j.cursur.2004.02.002) - DOI - PubMed
-
- Bell PD, Lapointe JY, Cardinal J, et al. Direct measurement of basolateral membrane potentials from cells of the macula densa. Am J Physiol. 1989;257(3 Pt 2):F463–F468. - PubMed
-
- Bell PD, Komlosi P, Zhang ZR, et al. ATP as a mediator of macula densa cell signalling. Purinergic Signal. 2009;5(4):461–471. (Available from: http://dx.doi.org/10.1007/s11302-009-9148-0) - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
