

Dynamic Stabilization with Active Locking Plates Delivers Faster, Stronger, and More Symmetric Fracture-Healing
- PMID: 26984914
- PMCID: PMC4788849
- DOI: 10.2106/JBJS.O.00705
Dynamic Stabilization with Active Locking Plates Delivers Faster, Stronger, and More Symmetric Fracture-Healing
Abstract
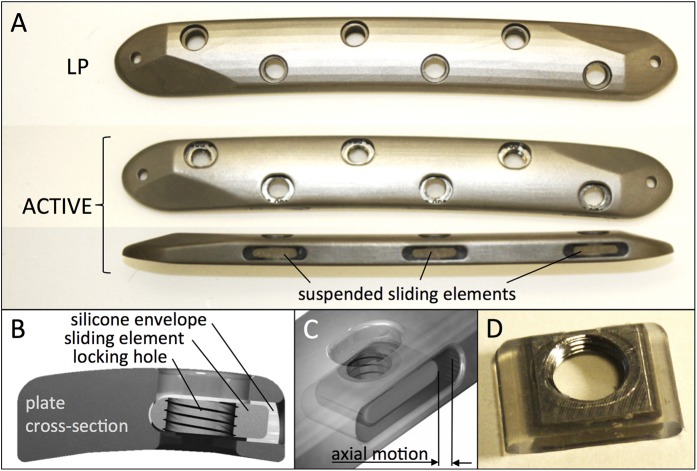
Background: Axial dynamization of fractures can promote healing, and overly stiff fixation can suppress healing. A novel technology, termed active plating, provides controlled axial dynamization by the elastic suspension of locking holes within the plate. This prospective, controlled animal study evaluated the effect of active plates on fracture-healing in an established ovine osteotomy model. We hypothesized that symmetric axial dynamization with active plates stimulates circumferential callus and delivers faster and stronger healing relative to standard locking plates.
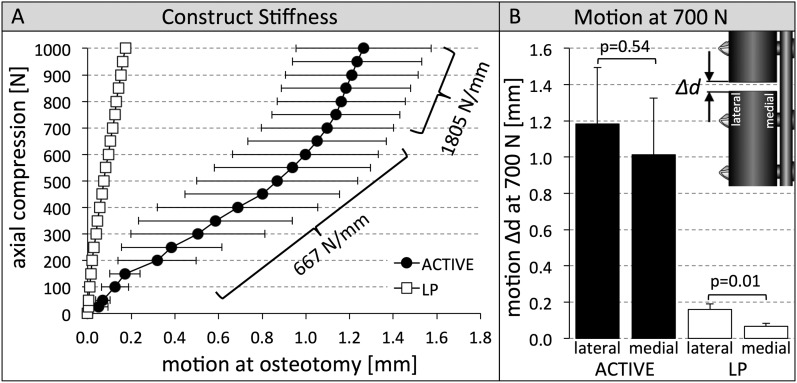
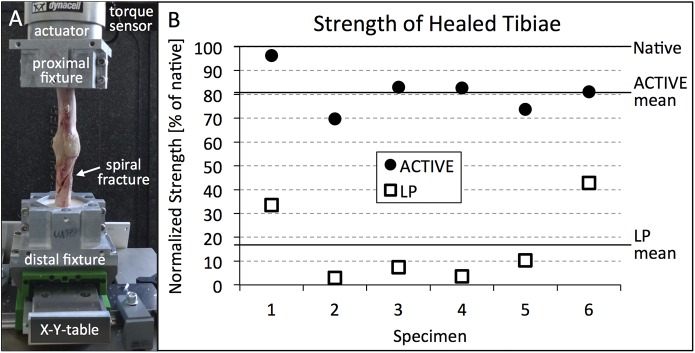
Methods: Twelve sheep were randomly assigned to receive a standard locking plate or an active locking plate for stabilization of a 3-mm tibial osteotomy gap. The only difference between plates was that locking holes of active plates were elastically suspended, allowing up to 1.5 mm of axial motion at the fracture. Fracture-healing was analyzed weekly on radiographs. After sacrifice at nine weeks postoperatively, callus volume and distribution were assessed by computed tomography. Finally, to determine their strength, healed tibiae and contralateral tibiae were tested in torsion until failure.
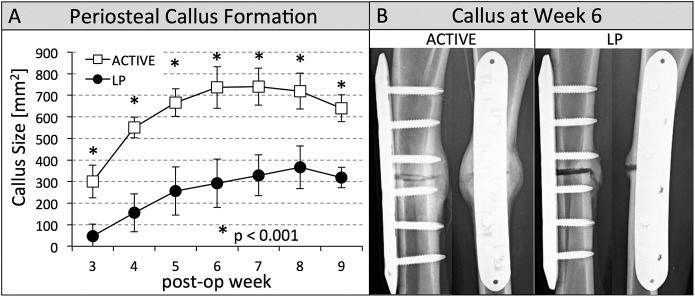
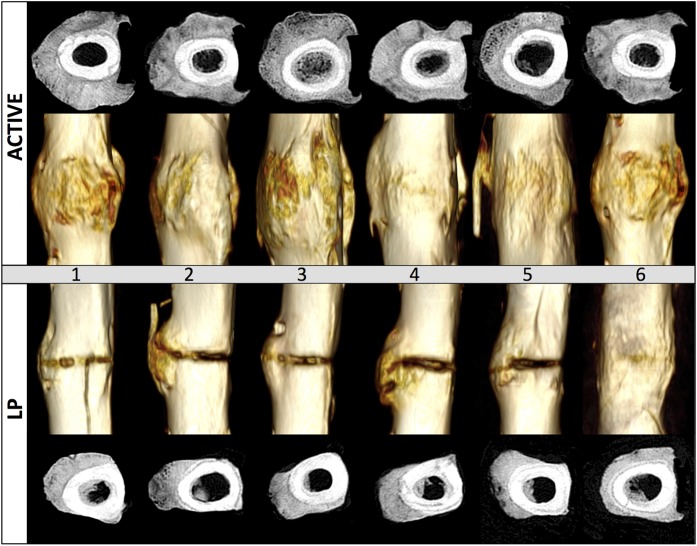
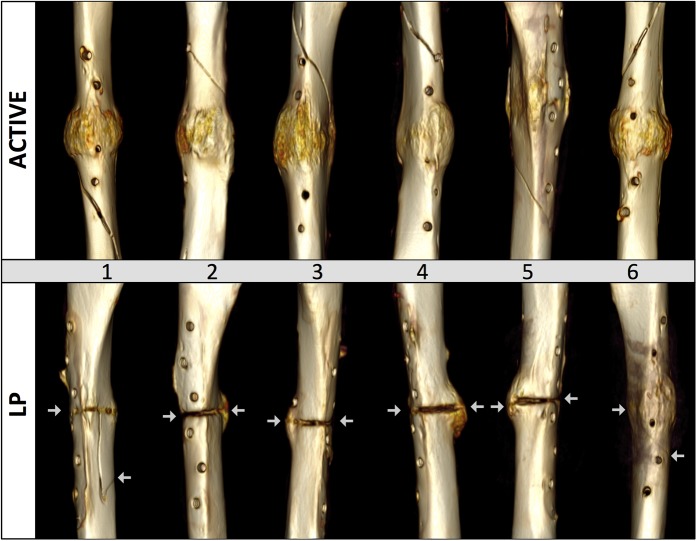
Results: At each follow-up, the active locking plate group had more callus (p < 0.001) than the standard locking plate group. At postoperative week 6, all active locking plate group specimens had bridging callus at the three visible cortices. In standard locking plate group specimens, only 50% of these cortices had bridged. Computed tomography demonstrated that all active locking plate group specimens and one of the six standard locking plate group specimens had developed circumferential callus. Torsion tests after plate removal demonstrated that active locking plate group specimens recovered 81% of their native strength and were 399% stronger than standard locking plate group specimens (p < 0.001), which had recovered only 17% of their native strength. All active locking plate group specimens failed by spiral fracture outside the callus zone, but standard locking plate group specimens fractured through the osteotomy gap.
Conclusions: Symmetric axial dynamization with active locking plates stimulates circumferential callus and yields faster and stronger healing than standard locking plates.
Clinical relevance: The stimulatory effect of controlled motion on fracture-healing by active locking plates has the potential to reduce healing complications and to shorten the time to return to function.
Copyright © 2016 by The Journal of Bone and Joint Surgery, Incorporated.
Figures
Comment in
-
The Challenge of Plate-Bone Construct Stiffness: A Swinging Pendulum: Commentary on an article by Michael Bottlang, PhD, et al.: "Dynamic Stabilization with Active Locking Plates Delivers Faster, Stronger, and More Symmetric Fracture-Healing".J Bone Joint Surg Am. 2016 Mar 16;98(6):e24. doi: 10.2106/JBJS.15.01337. J Bone Joint Surg Am. 2016. PMID: 26984924 No abstract available.
Similar articles
-
Dynamic Stabilization of Simple Fractures With Active Plates Delivers Stronger Healing Than Conventional Compression Plating.J Orthop Trauma. 2017 Feb;31(2):71-77. doi: 10.1097/BOT.0000000000000732. J Orthop Trauma. 2017. PMID: 27861456 Free PMC article.
-
Dynamization at the near cortex in locking plate osteosynthesis by means of dynamic locking screws: an experimental study of transverse tibial osteotomies in sheep.J Bone Joint Surg Am. 2015 Feb 4;97(3):208-15. doi: 10.2106/JBJS.M.00529. J Bone Joint Surg Am. 2015. PMID: 25653321
-
Dynamic Fixation of Humeral Shaft Fractures Using Active Locking Plates: A Prospective Observational Study.Iowa Orthop J. 2017;37:1-10. Iowa Orthop J. 2017. PMID: 28852327 Free PMC article.
-
Advances in Dynamization of Plate Fixation to Promote Natural Bone Healing.J Clin Med. 2024 May 14;13(10):2905. doi: 10.3390/jcm13102905. J Clin Med. 2024. PMID: 38792446 Free PMC article. Review.
-
Biomechanical and biological aspects of defect treatment in fractures using helical plates.Acta Chir Orthop Traumatol Cech. 2014;81(4):267-71. Acta Chir Orthop Traumatol Cech. 2014. PMID: 25137496 Review.
Cited by
-
Clinical outcomes in periarticular knee fractures with flexible fixation using far cortical locking screws in locking plate: a prospective study.Musculoskelet Surg. 2019 Aug;103(2):149-153. doi: 10.1007/s12306-018-0553-9. Epub 2018 Jul 2. Musculoskelet Surg. 2019. PMID: 29968233
-
Promoting bone callus formation by taking advantage of the time-dependent fracture gap strain modulation.Front Surg. 2024 May 2;11:1376441. doi: 10.3389/fsurg.2024.1376441. eCollection 2024. Front Surg. 2024. PMID: 38756355 Free PMC article. Review.
-
Combined electric and magnetic field therapy for bone repair and regeneration: an investigation in a 3-mm and an augmented 17-mm tibia osteotomy model in sheep.J Orthop Surg Res. 2023 Jun 24;18(1):454. doi: 10.1186/s13018-023-03910-6. J Orthop Surg Res. 2023. PMID: 37355696 Free PMC article.
-
Association of Gap Healing With Angle of Correction After Opening-Wedge High Tibial Osteotomy Without Bone Grafting.Orthop J Sports Med. 2021 May 11;9(5):23259671211002289. doi: 10.1177/23259671211002289. eCollection 2021 May. Orthop J Sports Med. 2021. PMID: 34026915 Free PMC article.
-
Comparative study of a novel proximal femoral bionic nail and three conventional cephalomedullary nails for reverse obliquity intertrochanteric fractures: a finite element analysis.Front Bioeng Biotechnol. 2024 Jun 13;12:1393154. doi: 10.3389/fbioe.2024.1393154. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38938983 Free PMC article.
References
-
- Claes LE, Heigele CA, Neidlinger-Wilke C, Kaspar D, Seidl W, Margevicius KJ, Augat P. Effects of mechanical factors on the fracture healing process. Clin Orthop Relat Res. 1998. October;355(Suppl):S132-47. - PubMed
-
- Foux A, Yeadon AJ, Uhthoff HK. Improved fracture healing with less rigid plates. A biomechanical study in dogs. Clin Orthop Relat Res. 1997. June;339:232-45. - PubMed
-
- Goodship AE, Kenwright J. The influence of induced micromovement upon the healing of experimental tibial fractures. J Bone Joint Surg Br. 1985. August;67(4):650-5. - PubMed
-
- Kenwright J, Richardson JB, Cunningham JL, White SH, Goodship AE, Adams MA, Magnussen PA, Newman JH. Axial movement and tibial fractures. A controlled randomised trial of treatment. J Bone Joint Surg Br. 1991. July;73(4):654-9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
