

Factors Affecting Physicians' Intentions to Communicate Personalized Prognostic Information to Cancer Patients at the End of Life: An Experimental Vignette Study
- PMID: 26985015
- PMCID: PMC4930679
- DOI: 10.1177/0272989X16638321
Factors Affecting Physicians' Intentions to Communicate Personalized Prognostic Information to Cancer Patients at the End of Life: An Experimental Vignette Study
Abstract
Purpose: To explore the effects of personalized prognostic information on physicians' intentions to communicate prognosis to cancer patients at the end of life, and to identify factors that moderate these effects.
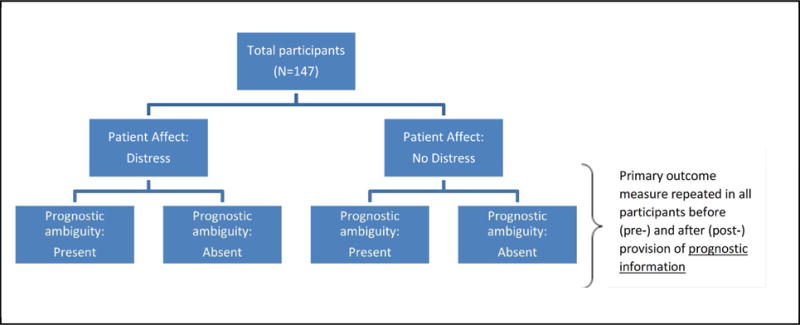
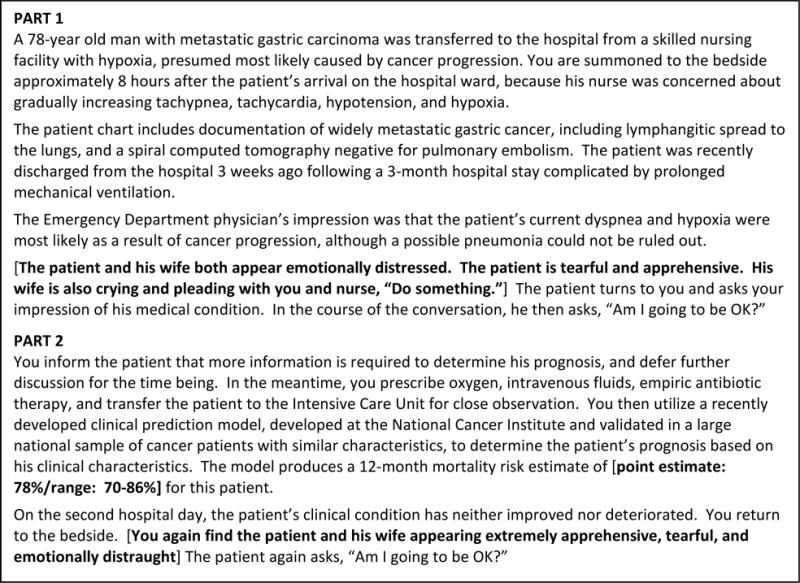
Methods: A factorial experiment was conducted in which 93 family medicine physicians were presented with a hypothetical vignette depicting an end-stage gastric cancer patient seeking prognostic information. Physicians' intentions to communicate prognosis were assessed before and after provision of personalized prognostic information, while emotional distress of the patient and ambiguity (imprecision) of the prognostic estimate were varied between subjects. General linear models were used to test the effects of personalized prognostic information, patient distress, and ambiguity on prognostic communication intentions, and potential moderating effects of 1) perceived patient distress, 2) perceived credibility of prognostic models, 3) physician numeracy (objective and subjective), and 4) physician aversion to risk and ambiguity.
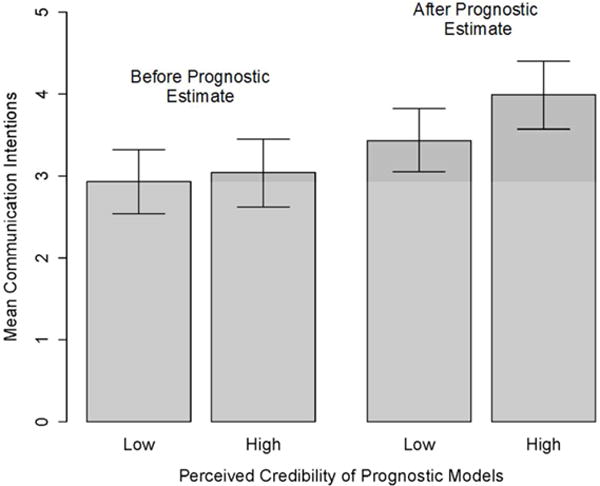
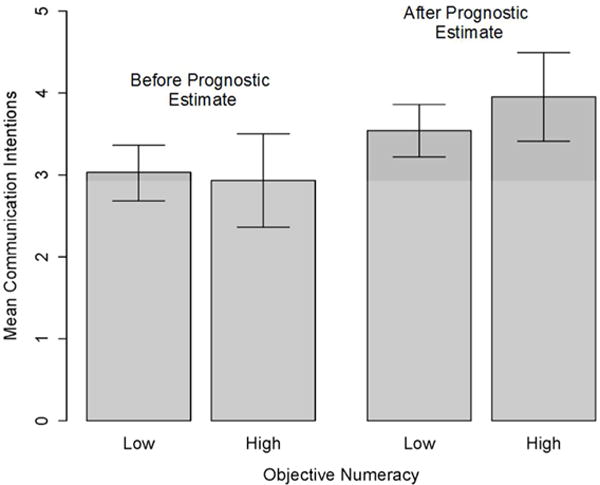
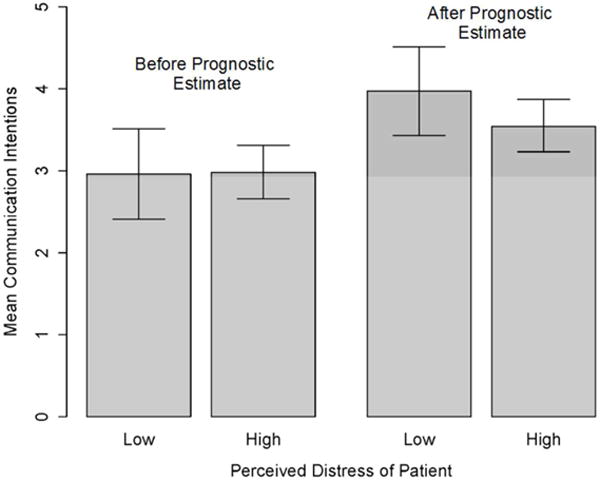
Results: Provision of personalized prognostic information increased prognostic communication intentions (P < 0.001, η(2) = 0.38), although experimentally manipulated patient distress and prognostic ambiguity had no effects. Greater change in communication intentions was positively associated with higher perceived credibility of prognostic models (P = 0.007, η(2) = 0.10), higher objective numeracy (P = 0.01, η(2) = 0.09), female sex (P = 0.01, η(2) = 0.08), and lower perceived patient distress (P = 0.02, η(2) = 0.07). Intentions to communicate available personalized prognostic information were positively associated with higher perceived credibility of prognostic models (P = 0.02, η(2) = 0.09), higher subjective numeracy (P = 0.02, η(2) = 0.08), and lower ambiguity aversion (P = 0.06, η(2) = 0.04).
Conclusions: Provision of personalized prognostic information increases physicians' prognostic communication intentions to a hypothetical end-stage cancer patient, and situational and physician characteristics moderate this effect. More research is needed to confirm these findings and elucidate the determinants of prognostic communication at the end of life.
Keywords: affect and emotion; numeracy; physician-patient communication; provider decision making; risk communication or risk perception; shared decision making.
© The Author(s) 2016.
Figures
References
-
- Clayton JM, Butow PN, Tattersall MH. The needs of terminally ill cancer patients versus those of caregivers for information regarding prognosis and end-of-life issues. Cancer. 2005;103(9):1957–1964. - PubMed
-
- Hancock K, Clayton JM, Parker SM, et al. Truth-telling in discussing prognosis in advanced life-limiting illnesses: a systematic review. Palliat Med. 2007;21(6):507–517. - PubMed
-
- Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284(19):2476–2482. - PubMed
-
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001;134(12):1096–1105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
