

The effects of vitamin K supplementation and vitamin K antagonists on progression of vascular calcification: ongoing randomized controlled trials
- PMID: 26985380
- PMCID: PMC4792621
- DOI: 10.1093/ckj/sfv146
The effects of vitamin K supplementation and vitamin K antagonists on progression of vascular calcification: ongoing randomized controlled trials
Abstract
Background: The extent and the progression of vascular calcification (VC) are independent predictors of cardiovascular risk in the haemodialysis population. Vitamin K is essential for the activation of matrix gla protein (MGP), a powerful inhibitor of tissue calcification. Functional vitamin K deficiency may contribute to the high VC burden in haemodialysis patients. In addition, haemodialysis patients are frequently treated with vitamin K antagonists, mainly to prevent stroke in atrial fibrillation, potentially compounding the cardiovascular risk in these already vulnerable patients. New oral anticoagulants (NOACs) are valuable alternatives to vitamin K antagonists in the general population, but their use in dialysis has been encumbered by substantial renal clearance. However, a recent pharmacokinetic study provided information on how to use rivaroxaban in haemodialysis patients.
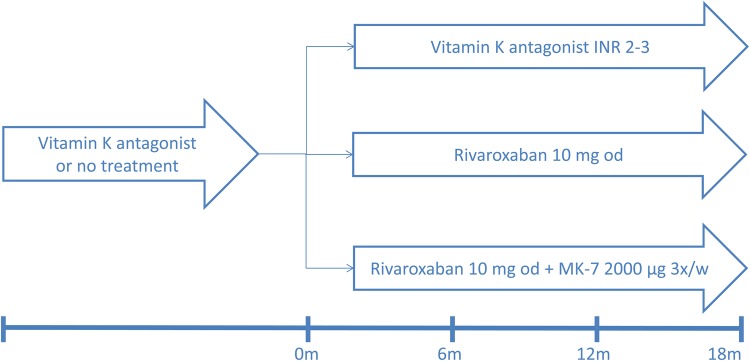
Methods: We conduct a randomized, prospective, multicentre, open-label interventional clinical trial that will include 117 chronic haemodialysis patients with non-valvular atrial fibrillation, treated with or candidates for treatment with vitamin K antagonists. Patients will be randomized to a vitamin K antagonist titrated weekly to an international normalized ratio between 2 and 3, a daily dose of rivaroxaban of 10 mg, or a daily dose of rivaroxaban 10 mg with a thrice weekly supplement of 2000 µg vitamin K2. Cardiac computed tomography, pulse wave velocity (PWV) measurements and MGP sampling will be performed at baseline, 6 months, 12 months and 18 months. Primary endpoints include progression of coronary artery and thoracic aorta calcification and changes in PWV. Secondary endpoints are progression of aortic and mitral valve calcification, all-cause mortality, major adverse cardiovascular events, stroke and bleeding. The ClinicalTrials.gov database was searched to retrieve related trials.
Results: Seven trials, three of which are performed in the haemodialysis population, evaluate whether pharmacological doses of vitamin K1 or K2 retard progression of VC. Five studies compare the effect of warfarin and NOACs on progression of VC, the present study being the only conducted in the dialysis population.
Conclusion: Vitamin K deficiency may be a modifiable cardiovascular risk factor in the haemodialysis population. Conversely, vitamin K antagonists may aggravate VC burden in haemodialysis patients. Several ongoing trials may provide an answer to these questions in the near future.
Keywords: haemodialysis; rivaroxaban; vascular calcifications; vitamin K; vitamin K antagonists.
References
-
- Bellasi A, Raggi P. Vascular imaging in chronic kidney disease. Curr Opin Nephrol Hypertens 2012; 21: 382–388 - PubMed
-
- Brandenburg VM, Schurgers LJ, Kaesler N, et al. Prevention of vasculopathy by vitamin K supplementation: can we turn fiction into fact? Atherosclerosis 2015; 240: 10–16 - PubMed
-
- Cranenburg ECM, Schurgers LJ, Uiterwijk HH, et al. Vitamin K intake and status are low in hemodialysis patients. Kidney Int 2012; 82: 605–610 - PubMed
-
- Caluwé R, Vandecasteele S, Van Vlem B, et al. Vitamin K2 supplementation in haemodialysis patients: a randomized dose-finding study. Nephrol Dial Transplant 2013; 29: 1385–1390 - PubMed
-
- Kaesler N, Magdeleyns E, Herfs M, et al. Impaired vitamin K recycling in uremia is rescued by vitamin K supplementation. Kidney Int 2014; 86: 286–293 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
