

Ankylosing spondylitis diagnosis in US patients with back pain: identifying providers involved and factors associated with rheumatology referral delay
- PMID: 26987341
- PMCID: PMC4914524
- DOI: 10.1007/s10067-016-3231-z
Ankylosing spondylitis diagnosis in US patients with back pain: identifying providers involved and factors associated with rheumatology referral delay
Abstract
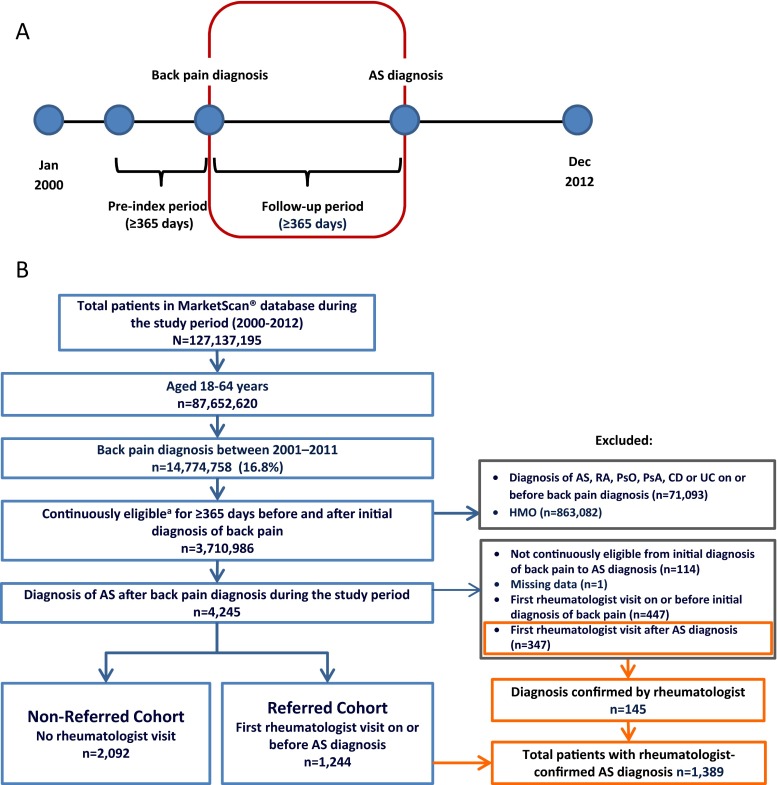
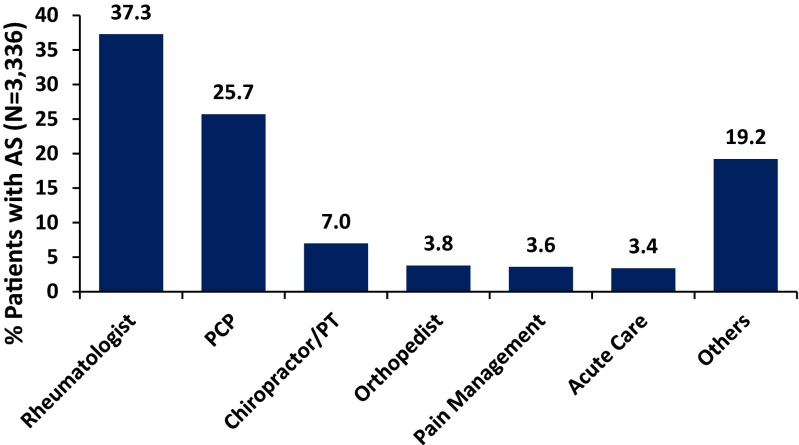
This study aimed to identify providers involved in diagnosing ankylosing spondylitis (AS) following back pain diagnosis in the USA and to identify factors leading to the delay in rheumatology referrals. The Truven Health MarketScan® US Commercial Database was searched for patients aged 18-64 years with back pain diagnosis in a non-rheumatology setting followed by AS diagnosis in any setting during January 2000-December 2012. Patients with a rheumatologist visit on or before AS diagnosis were considered referred. Cox regression was used to determine factors associated with referral time after adjusting for age, sex, comorbidities, physician specialty, drug therapy, and imaging procedures. Of 3336 patients included, 1244 (37 %) were referred to and diagnosed by rheumatologists; the others were diagnosed in primary care (25.7 %), chiropractic/physical therapy (7 %), orthopedic surgery (3.8 %), pain clinic (3.6 %), acute care (3.4 %), and other (19.2 %) settings. Median time from back pain diagnosis to rheumatology referral was 307 days and from first rheumatologist visit to AS diagnosis was 28 days. Referred patients were more likely to be younger (hazard ratio [HR] = 0.986; p < 0.0001), male (HR = 1.15; p = 0.0163), diagnosed with uveitis (HR = 1.49; p = 0.0050), referred by primary care physicians (HR = 1.96; p < 0.0001), prescribed non-steroidal anti-inflammatory drugs (HR = 1.55; p < 0.0001), disease-modifying antirheumatic drugs (HR = 1.33; p < 0.0001), and tumor necrosis factor inhibitors (HR = 1.40; p = 0.0036), and to have had spinal/pelvic X-ray prior to referral (HR = 1.28; p = 0.0003). During 2000-2012, most patients with AS were diagnosed outside of rheumatology practices. The delay before referral to rheumatology was 10 months; AS diagnosis generally followed within a month. Earlier referral of patients with AS signs and symptoms may lead to more timely diagnosis and appropriate treatment.
Keywords: Ankylosing spondylitis; Anti-TNF; Diagnostic delay; Referral strategies; Treatment patterns.
Figures

References
-
- Feldtkeller E, Khan MA, van der Heijde D, van der Linden S, Braun J. Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis. Rheumatol Int. 2003;23:61–66. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
