

Outcome of patients with local recurrent gynecologic malignancies after resection combined with intraoperative electron radiation therapy (IOERT)
- PMID: 26988089
- PMCID: PMC4797348
- DOI: 10.1186/s13014-016-0622-x
Outcome of patients with local recurrent gynecologic malignancies after resection combined with intraoperative electron radiation therapy (IOERT)
Abstract
Background: Treatment of recurrent gynecologic cancer is a challenging issue. Aim of the study was to investigate clinical features and outcomes of patients with recurrent gynecologic malignancies who underwent resection including IOERT (intraoperative electron radiation therapy) with regard to clinical outcome and potential predictive factors or subgroups that benefit most from this radical treatment regime.
Methods: A total of 36 patients with recurrent gynecologic malignancies (cervical (n = 18), endometrial (n = 12) or vulvar cancer (n = 6)) were retrospectively identified through hospital databases in accordance with institutional ethical policies. Patient characteristics and outcomes were assessed. Survival data was analyzed using the Kaplan-Meier-method and log-rank-test, categorical variables were analyzed with chi-square-method.
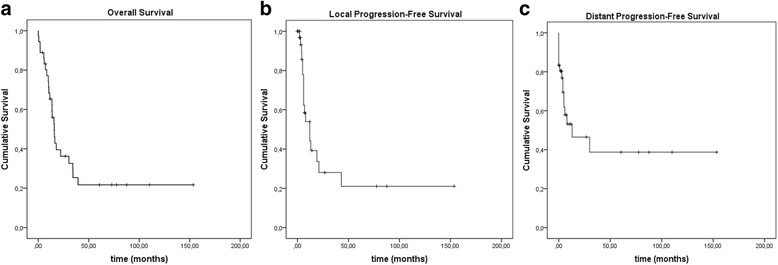
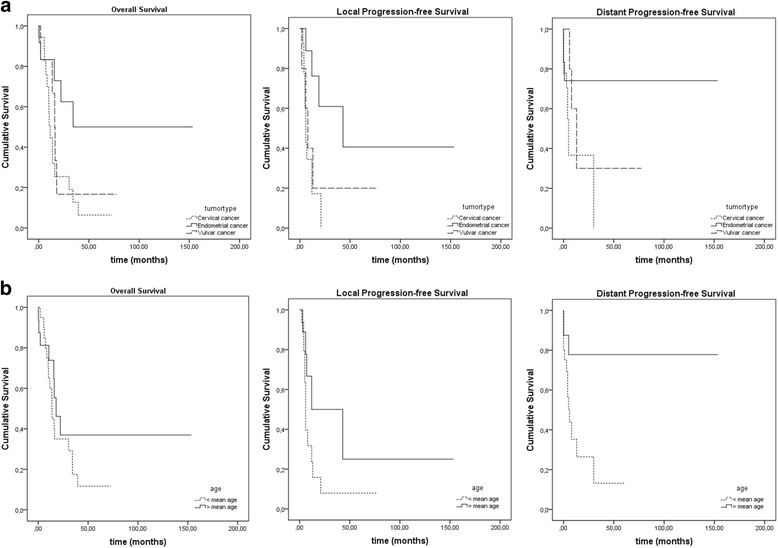
Results: For the entire cohort 1-/2-/5-year Overall Survival (OS) was 65.3 %/36.2 %/21.7 %. Patients with endometrial, cervical, and vulvar carcinoma had a 1-/2-/5-year OS of 83.3 %/62.5 %/50 %, 44.5 %/25.4 %/6.4 %, and 83.3 %/16.7 %/16.7 %, respectively. Patients with endometrial carcinoma showed a significantly better OS (p = 0.038). 1-/2-/5-year Local Progression-free Survival (LPFS) for the entire cohort was 44.1 %/28 %/21 % with 76.2 %/61 %/40.6 % for endometrial, 17.2 %/0 %/0 % for cervical, and 40 %/20 %/20 % for vulvar cancer, respectively. Patients with endometrial cancer showed a significantly (p = 0.017) and older patients a trend (p = 0.059) for a better LPFS. 1-/2-/5-year Distant Progression-free Survival (DPFS) for the entire cohort was 53.1 %/46.5 %/38.7 % with 74.1 %/74.1 %/74.1 % for endometrial, 36.7 %/36.7 %/0 % for cervical, and 60 %/30 %/30 % for vulvar cancer, respectively. There was a significantly better DPFS for older patients (p = 0.015) and a trend for a better DPFS for patients with endometrial carcinoma (p = 0.075).
Conclusion: The radical procedure of resection combined with IOERT seems to be a valid curative treatment option for patients with recurrent endometrial carcinoma with 5-year survival rates of 50 %. For patients with cervical or vulvar cancer this treatment should be considered a rather palliative one and must be weighted carefully against other treatment options like chemotherapy, targeted therapies or new highly conformal radiotherapy techniques.
Keywords: Cervical cancer; Endometrial cancer; IOERT; Pelvic exenteration; Recurrent gynecologic cancer; Vulvar cancer.
Figures
References
-
- Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Wárlám-Rodenhuis CC, De Winter KA, Lutgens LC, van den Bergh AC, van de Steen-Banasik E, Beerman H, van Lent M. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet (London, England). 2000;355:1404–11. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
