

A Randomized, Double-Blind, Active- and Placebo-Controlled Efficacy and Safety Study of Arhalofenate for Reducing Flare in Patients With Gout
- PMID: 26989892
- PMCID: PMC5129473
- DOI: 10.1002/art.39684
A Randomized, Double-Blind, Active- and Placebo-Controlled Efficacy and Safety Study of Arhalofenate for Reducing Flare in Patients With Gout
Abstract
Objective: Arhalofenate is a novel antiinflammatory uricosuric agent. The objective of this study was to evaluate its antiflare activity in patients with gout.
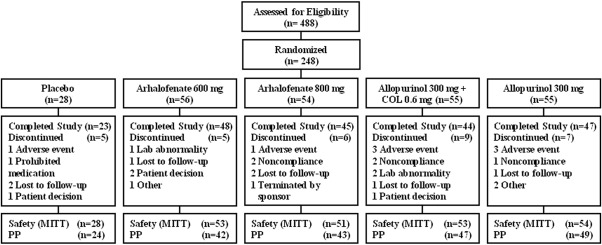
Methods: This was a 12-week, randomized, double-blind, controlled phase IIb study. Eligible patients had had ≥3 flares of gout during the previous year, had discontinued urate-lowering therapy and colchicine, and had a serum uric acid (UA) level of 7.5-12 mg/dl. Patients were randomly assigned at a 2:2:2:2:1 ratio to receive 600 mg arhalofenate, 800 mg arhalofenate, 300 mg allopurinol, 300 mg allopurinol plus 0.6 mg colchicine, or placebo once a day. The primary outcome measure was the flare incidence (number of flares divided by time of exposure). The serum UA level was a secondary outcome measure.
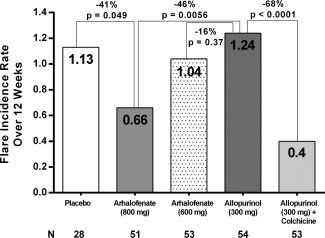
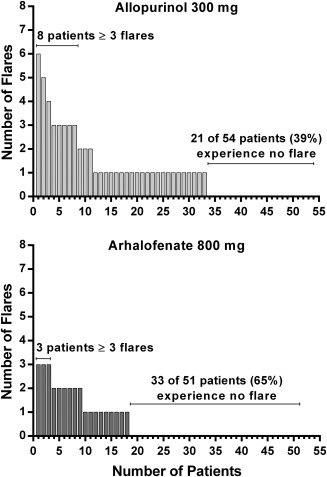
Results: A total of 239 gout patients were randomized and took at least 1 dose of study medication. The primary outcome measure comparing flare incidence between 800 mg arhalofenate and 300 mg allopurinol was achieved, with a 46% decrease in the 800 mg arhalofenate group (0.66 versus 1.24; P = 0.0056). Treatment with 800 mg arhalofenate was also significantly better than placebo (P = 0.049) and not significantly different from treatment with 300 mg allopurinol plus 0.6 mg colchicine (P = 0.091). Mean changes in serum UA level were -12.5% with 600 mg arhalofenate and -16.5% with 800 mg arhalofenate (P = 0.001 and P = 0.0001, respectively, versus -0.9% with placebo). There were no meaningful differences in adverse events (AEs) between groups, and there were no serious AEs related to arhalofenate. Urinary calculus occurred in 1 patient receiving 300 mg allopurinol. No abnormal serum creatinine values >1.5-fold the baseline value were observed in the arhalofenate-treated groups.
Conclusion: Arhalofenate at a dosage of 800 mg decreased gout flares significantly compared to allopurinol at a dosage of 300 mg. Arhalofenate was well tolerated and appeared safe. Arhalofenate is the first urate-lowering antiflare therapy.
Trial registration: ClinicalTrials.gov NCT02063997.
© 2016 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of the American College of Rheumatology.
Figures
Comment in
-
Editorial: Pursuit of a Dual-Benefit Antigout Drug: A First Look at Arhalofenate.Arthritis Rheumatol. 2016 Aug;68(8):1793-6. doi: 10.1002/art.39687. Arthritis Rheumatol. 2016. PMID: 26990165 Free PMC article. No abstract available.
-
Crystal arthritis: Arhalofenate safely prevents gout flare.Nat Rev Rheumatol. 2016 May;12(5):252. doi: 10.1038/nrrheum.2016.53. Epub 2016 Apr 7. Nat Rev Rheumatol. 2016. PMID: 27052485 No abstract available.
References
-
- Edwards NL, Sundy JS, Forsythe A, Blume S, Pan F, Becker MA. Work productivity loss due to flares in patients with chronic gout refractory to conventional therapy. J Med Econ 2011;14:10–5. - PubMed
-
- Brook RA, Forsythe A, Smeeding JE, Edwards NL. Chronic gout: epidemiology, disease progression, treatment and disease burden. Curr Med Res Opin 2010;26:2813–21. - PubMed
-
- Stamp LK. Safety profile of anti‐gout agents: an update. Curr Opin Rheumatol 2014;26:162–8. - PubMed
-
- Smith E, Hoy D, Cross M, Merriman TR, Vos T, Buchbinder R, et al. The global burden of gout: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73:1470–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
