

Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis
- PMID: 26990957
- PMCID: PMC5069642
- DOI: 10.1002/bjs.10147
Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis
Abstract
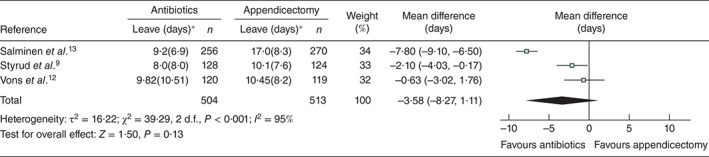
Background: For more than a century, appendicectomy has been the treatment of choice for appendicitis. Recent trials have challenged this view. This study assessed the benefits and harms of antibiotic therapy compared with appendicectomy in patients with non-perforated appendicitis.
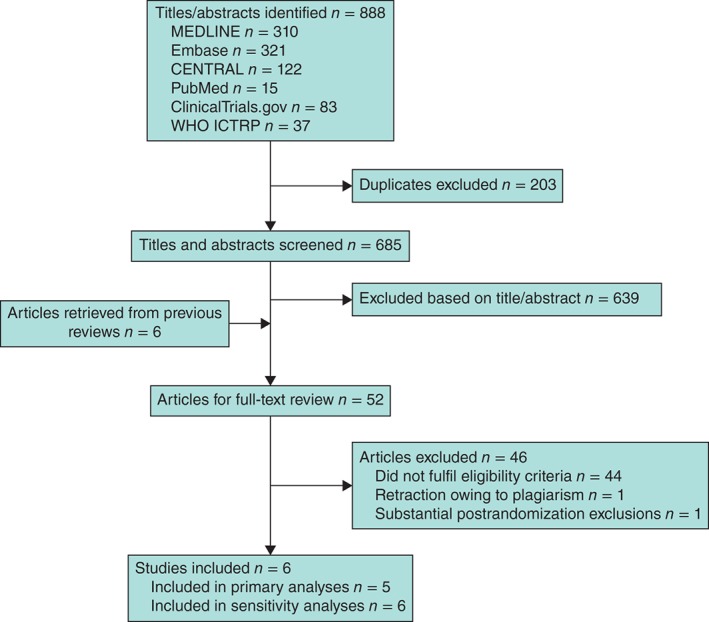
Methods: A comprehensive search was conducted for randomized trials comparing antibiotic therapy with appendicectomy in patients with non-perforated appendicitis. Key outcomes were analysed using random-effects meta-analysis, and the quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
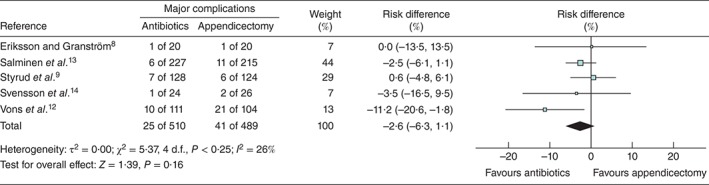
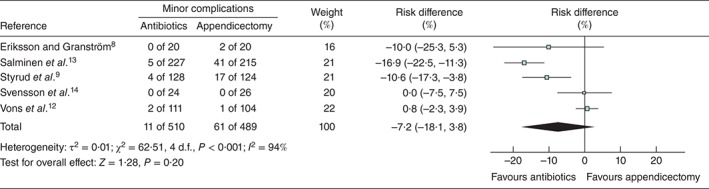
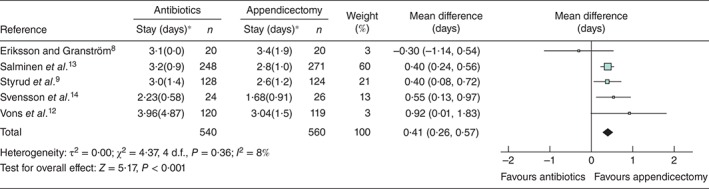
Results: Five studies including 1116 patients reported major complications in 25 (4·9 per cent) of 510 patients in the antibiotic and 41 (8·4 per cent) of 489 in the appendicectomy group: risk difference -2·6 (95 per cent c.i. -6·3 to 1·1) per cent (low-quality evidence). Minor complications occurred in 11 (2·2 per cent) of 510 and 61 (12·5 per cent) of 489 patients respectively: risk difference -7·2 (-18·1 to 3·8) per cent (very low-quality evidence). Of 550 patients in the antibiotic group, 47 underwent appendicectomy within 1 month: pooled estimate 8·2 (95 per cent c.i. 5·2 to 11·8) per cent (high-quality evidence). Within 1 year, appendicitis recurred in 114 of 510 patients in the antibiotic group: pooled estimate 22·6 (15·6 to 30·4) per cent (high-quality evidence). For every 100 patients with non-perforated appendicitis, initial antibiotic therapy compared with prompt appendicectomy may result in 92 fewer patients receiving surgery within the first month, and 23 more experiencing recurrent appendicitis within the first year.
Conclusion: The choice of medical versus surgical management in patients with clearly uncomplicated appendicitis is value- and preference-dependent, suggesting a change in practice towards shared decision-making is necessary.
© 2016 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Comment in
-
Are Antibiotics a Feasible Alternative to Surgery for Acute Appendicitis?Ann Emerg Med. 2017 Mar;69(3):362-363. doi: 10.1016/j.annemergmed.2016.04.019. Epub 2016 May 4. Ann Emerg Med. 2017. PMID: 27157453 No abstract available.
-
[Antibiotic treatment versus appendectomy for non-perforated appendicitis : Results of a meta-analysis].Chirurg. 2016 Sep;87(9):795. doi: 10.1007/s00104-016-0269-z. Chirurg. 2016. PMID: 27503617 German. No abstract available.
-
Antibiotic treatment of appendicitis.J Pediatr. 2016 Sep;176:221-4. doi: 10.1016/j.jpeds.2016.06.074. J Pediatr. 2016. PMID: 27568256 No abstract available.
References
-
- Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990; 132: 910–925. - PubMed
-
- Masoomi H, Nguyen NT, Dolich MO, Mills S, Carmichael JC, Stamos MJ. Laparoscopic appendectomy trends and outcomes in the United States: data from the Nationwide Inpatient Sample (NIS), 2004–2011. Am Surg 2014; 80: 1074–1077. - PubMed
-
- Fitz RH. Perforating inflammation of the vermiform appendix: with special reference to its early diagnosis and treatment. Am J Med Sci 1886; 92: 321–346.
-
- McBurney C. Experience with early operative interference in cases of disease of the vermiform appendix. NY Med J 1889; 50: 676–684.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
