

Comparing Risk Factor Profiles between Intracerebral Hemorrhage and Ischemic Stroke in Chinese and White Populations: Systematic Review and Meta-Analysis
- PMID: 26991497
- PMCID: PMC4798495
- DOI: 10.1371/journal.pone.0151743
Comparing Risk Factor Profiles between Intracerebral Hemorrhage and Ischemic Stroke in Chinese and White Populations: Systematic Review and Meta-Analysis
Abstract
Background: Chinese populations have a higher proportion of intracerebral hemorrhage (ICH) in total strokes. However, the reasons are not fully understood.
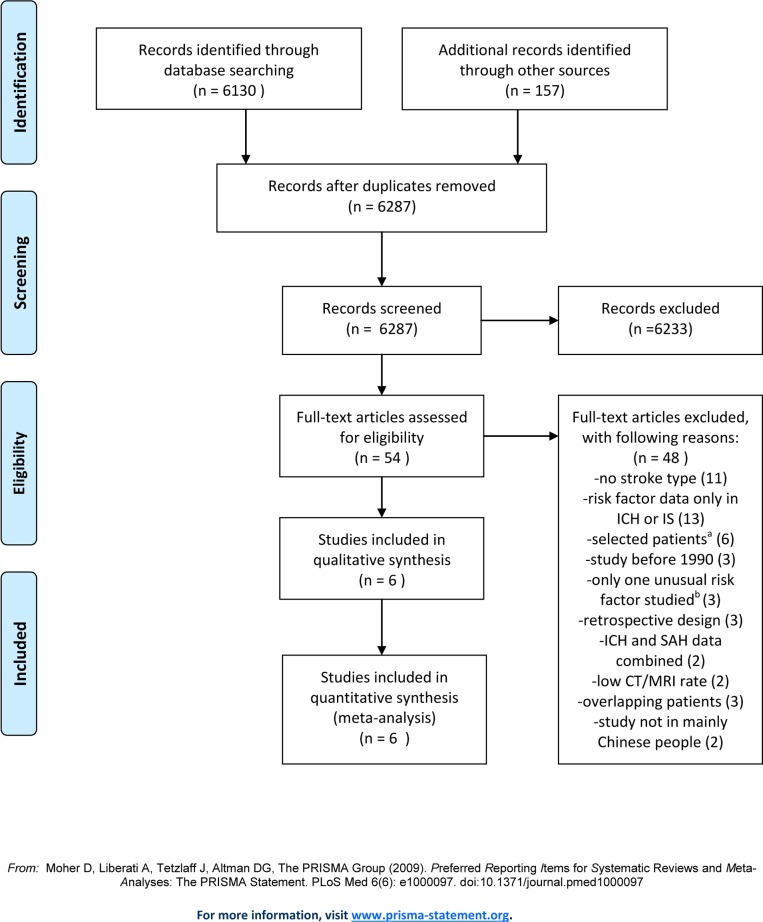
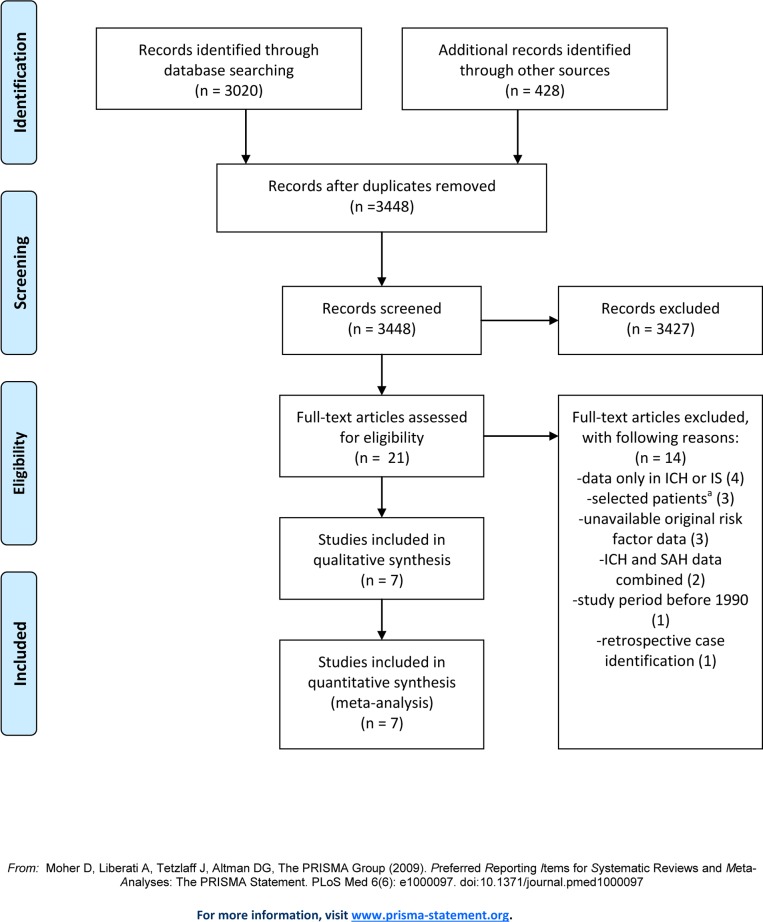
Methods: To assess the differences in frequency of major risk factors between ICH and ischemic stroke (IS) in Chinese versus white populations of European descent, we systematically sought studies conducted since 1990 that compared frequency of risk factors between ICH and IS in Chinese or white populations. For each risk factor, in Chinese and Whites separately, we calculated study-specific and random effects pooled prevalence and odds ratios (ORs) for ICH versus IS.
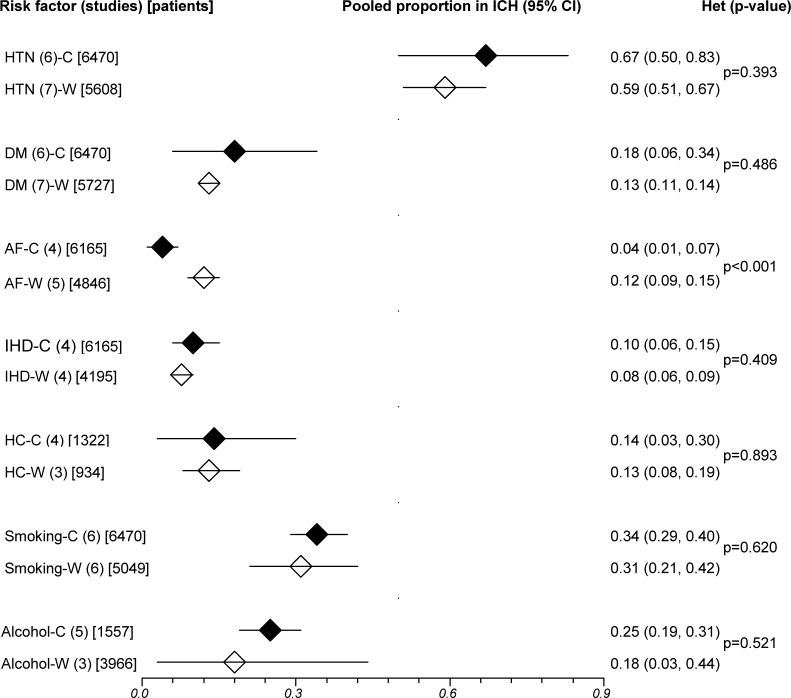
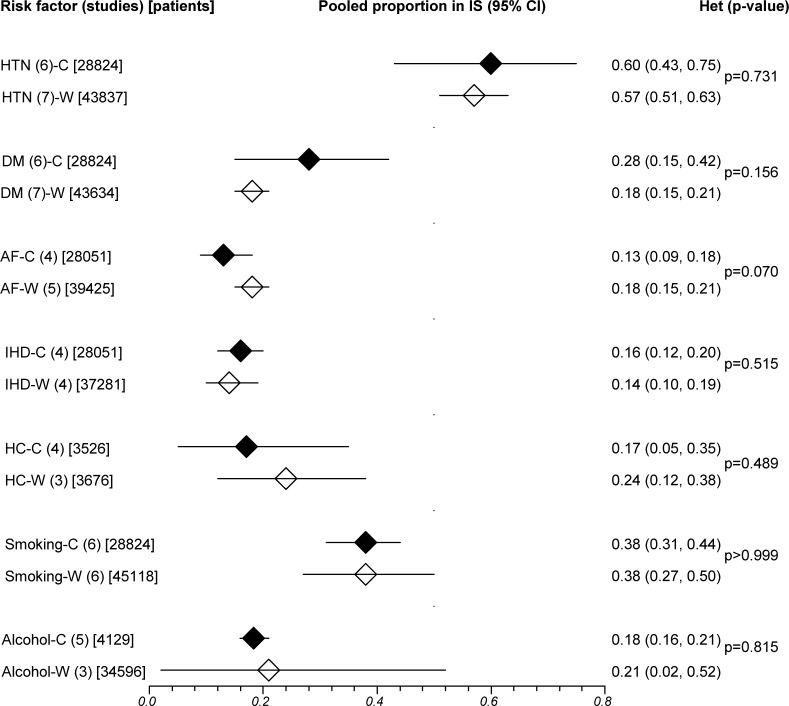
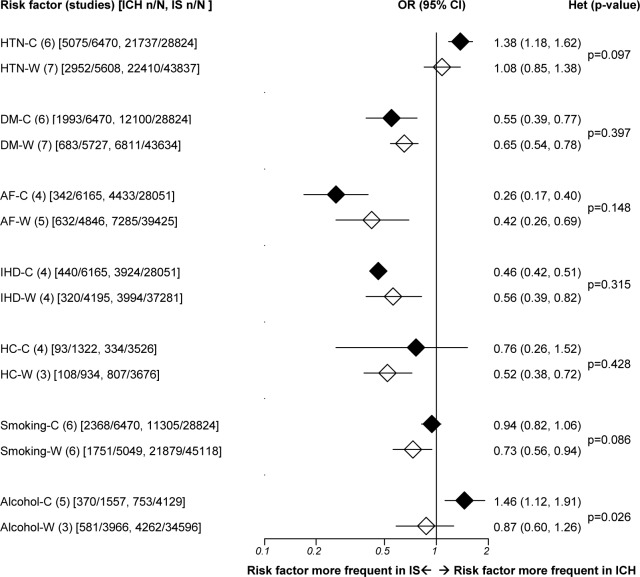
Results: Six studies among 36,190 Chinese, and seven among 52,100 white stroke patients studied hypertension, diabetes, atrial fibrillation (AF), ischemic heart disease (IHD), hypercholesterolemia, smoking and alcohol. Pooled prevalence of AF was significantly lower in Chinese. Pooled ORs for ICH versus IS were mostly similar in Chinese and Whites. However, in Chinese--but not Whites--mean age was lower (62 versus 69 years), while hypertension and alcohol were significantly more frequent in ICH than IS (ORs 1.38, 95% CI 1.18-1.62, and 1.46, 1.12-1.91). Hypercholesterolemia and smoking were significantly less frequent in ICH in Whites, but not Chinese, while IHD, AF and diabetes were less frequent in ICH in both.
Conclusions: Different risk factor distributions in ICH and IS raise interesting possibilities about variation in mechanisms underlying the different distributions of pathological types of stroke between Chinese and Whites. Further analyses in large, prospective studies, including adjustment for potential confounders, are needed to consolidate and extend these findings.
Conflict of interest statement
Figures
References
-
- Asch CJJV, Luites MJA, Rinkel GJE, Tweel IVD, Algra A, Klijn CJM. Incidence, case fatality, and functional outcome of intracranial haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 2010;9:167–176. 10.1016/S1474-4422(09)70340-0 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
