

Multicentre multi-device hybrid imaging study of coronary artery disease: results from the EValuation of INtegrated Cardiac Imaging for the Detection and Characterization of Ischaemic Heart Disease (EVINCI) hybrid imaging population
- PMID: 26992419
- PMCID: PMC5841878
- DOI: 10.1093/ehjci/jew038
Multicentre multi-device hybrid imaging study of coronary artery disease: results from the EValuation of INtegrated Cardiac Imaging for the Detection and Characterization of Ischaemic Heart Disease (EVINCI) hybrid imaging population
Abstract
Aims: Hybrid imaging provides a non-invasive assessment of coronary anatomy and myocardial perfusion. We sought to evaluate the added clinical value of hybrid imaging in a multi-centre multi-vendor setting.
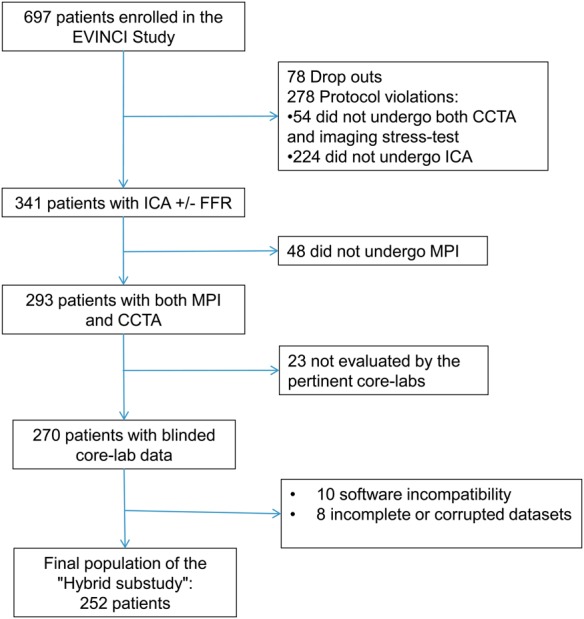
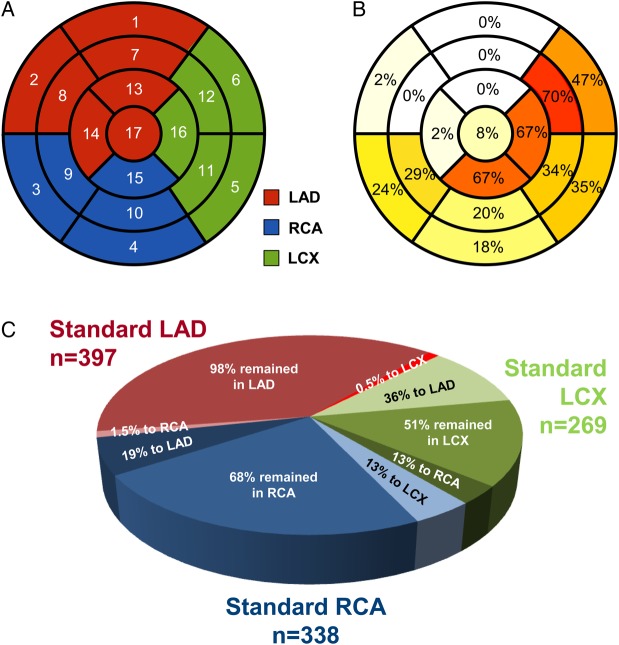
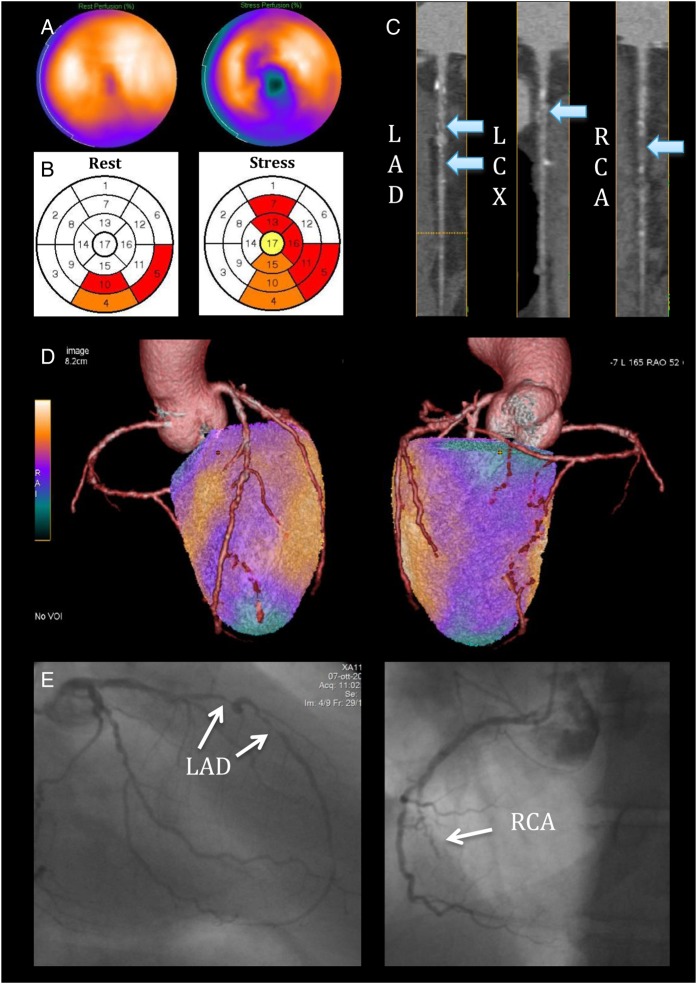
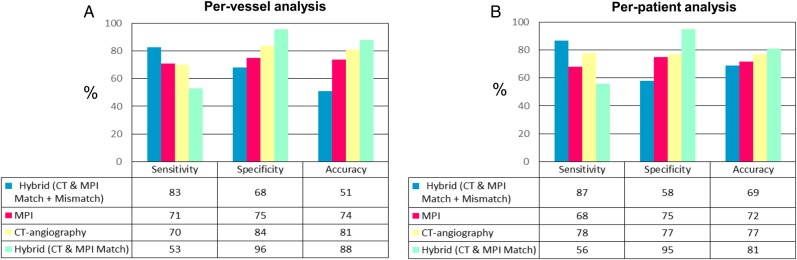
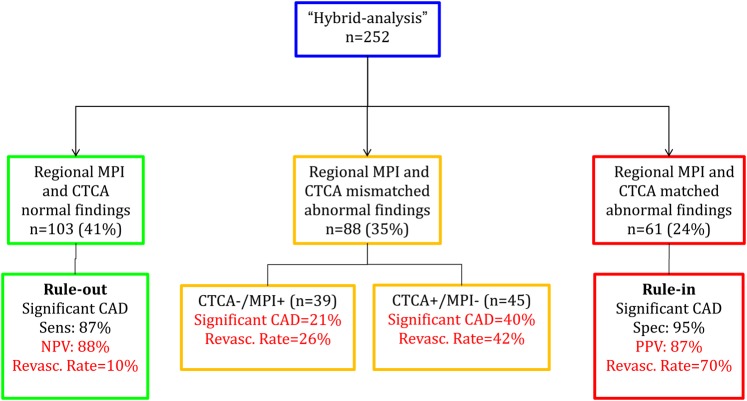
Methods and results: Fourteen centres enrolled 252 patients with stable angina and intermediate (20-90%) pre-test likelihood of coronary artery disease (CAD) who underwent myocardial perfusion scintigraphy (MPS), CT coronary angiography (CTCA), and quantitative coronary angiography (QCA) with fractional flow reserve (FFR). Hybrid MPS/CTCA images were obtained by 3D image fusion. Blinded core-lab analyses were performed for CTCA, MPS, QCA and hybrid datasets. Hemodynamically significant CAD was ruled-in non-invasively in the presence of a matched finding (myocardial perfusion defect co-localized with stenosed coronary artery) and ruled-out with normal findings (both CTCA and MPS normal). Overall prevalence of significant CAD on QCA (>70% stenosis or 30-70% with FFR≤0.80) was 37%. Of 1004 pathological myocardial segments on MPS, 246 (25%) were reclassified from their standard coronary distribution to another territory by hybrid imaging. In this respect, in 45/252 (18%) patients, hybrid imaging reassigned an entire perfusion defect to another coronary territory, changing the final diagnosis in 42% of the cases. Hybrid imaging allowed non-invasive CAD rule-out in 41%, and rule-in in 24% of patients, with a negative and positive predictive value of 88% and 87%, respectively.
Conclusion: In patients at intermediate risk of CAD, hybrid imaging allows non-invasive co-localization of myocardial perfusion defects and subtending coronary arteries, impacting clinical decision-making in almost one every five subjects.
Keywords: CT coronary angiography; Coronary artery disease; Hybrid imaging; Myocardial perfusion scintigraphy.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
Similar articles
-
Hemodynamic impact of coronary stenosis using computed tomography: comparison between noninvasive fractional flow reserve and 3D fusion of coronary angiography with stress myocardial perfusion.Int J Cardiovasc Imaging. 2019 Sep;35(9):1733-1743. doi: 10.1007/s10554-019-01618-5. Epub 2019 May 9. Int J Cardiovasc Imaging. 2019. PMID: 31073698 Free PMC article.
-
Fusion of CT coronary angiography and whole-heart dynamic 3D cardiac MR perfusion: building a framework for comprehensive cardiac imaging.Int J Cardiovasc Imaging. 2018 Apr;34(4):649-660. doi: 10.1007/s10554-017-1260-6. Epub 2017 Oct 28. Int J Cardiovasc Imaging. 2018. PMID: 29080955
-
CT myocardial perfusion and coronary CT angiography: Influence of coronary calcium on a stress-rest protocol.J Cardiovasc Comput Tomogr. 2016 May-Jun;10(3):215-20. doi: 10.1016/j.jcct.2016.01.013. Epub 2016 Jan 30. J Cardiovasc Comput Tomogr. 2016. PMID: 26869367
-
Hybrid Imaging in Ischemic Heart Disease.Rev Esp Cardiol (Engl Ed). 2018 May;71(5):382-390. doi: 10.1016/j.rec.2017.11.023. Epub 2018 Jan 10. Rev Esp Cardiol (Engl Ed). 2018. PMID: 29329818 Review. English, Spanish.
-
CT-based myocardial ischemia evaluation: quantitative angiography, transluminal attenuation gradient, myocardial perfusion, and CT-derived fractional flow reserve.Int J Cardiovasc Imaging. 2016 Jun;32 Suppl 1:1-19. doi: 10.1007/s10554-015-0825-5. Epub 2015 Dec 14. Int J Cardiovasc Imaging. 2016. PMID: 26667445 Review.
Cited by
-
Computed Tomography Angiography Identified High-Risk Coronary Plaques: From Diagnosis to Prognosis and Future Management.Diagnostics (Basel). 2024 Aug 1;14(15):1671. doi: 10.3390/diagnostics14151671. Diagnostics (Basel). 2024. PMID: 39125547 Free PMC article. Review.
-
CT Myocardial Perfusion Imaging: A New Frontier in Cardiac Imaging.Biomed Res Int. 2018 Oct 14;2018:7295460. doi: 10.1155/2018/7295460. eCollection 2018. Biomed Res Int. 2018. PMID: 30406139 Free PMC article. Review.
-
Diagnostic Performance of Hybrid Cardiac Imaging Methods for Assessment of Obstructive Coronary Artery Disease Compared With Stand-Alone Coronary Computed Tomography Angiography: A Meta-Analysis.JACC Cardiovasc Imaging. 2018 Apr;11(4):589-599. doi: 10.1016/j.jcmg.2017.05.020. Epub 2017 Aug 16. JACC Cardiovasc Imaging. 2018. PMID: 28823745 Free PMC article.
-
Incremental prognostic value of hybrid [15O]H2O positron emission tomography-computed tomography: combining myocardial blood flow, coronary stenosis severity, and high-risk plaque morphology.Eur Heart J Cardiovasc Imaging. 2020 Oct 1;21(10):1105-1113. doi: 10.1093/ehjci/jeaa192. Eur Heart J Cardiovasc Imaging. 2020. PMID: 32959061 Free PMC article.
-
Noninvasive CT-based hemodynamic assessment of coronary lesions derived from fast computational analysis: a comparison against fractional flow reserve.Eur Radiol. 2019 Apr;29(4):2117-2126. doi: 10.1007/s00330-018-5781-8. Epub 2018 Oct 15. Eur Radiol. 2019. PMID: 30324382
References
-
- Task Force Members. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949–3003. - PubMed
-
- Gaemperli O, Schepis T, Valenta I, Koepfli P, Husmann L, Scheffel H et al. . Functionally relevant coronary artery disease: comparison of 64-section CT angiography with myocardial perfusion SPECT. Radiology 2008;248:414–23. - PubMed
-
- Tonino PA, Fearon WF, De Bruyne B, Oldroyd KG, Leesar MA, Ver Lee PN et al. . Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol 2010;55:2816–21. - PubMed
-
- Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM et al. . Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation 2008;117:1283–91. - PubMed
-
- De Bruyne B, Fearon WF, Pijls NH, Barbato E, Tonino P, Piroth Z et al. . Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med 2014;371:1208–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
