

Long-term echocardiographic follow-up of untreated 2+ functional tricuspid regurgitation in patients undergoing mitral valve surgery
- PMID: 26993477
- PMCID: PMC4986742
- DOI: 10.1093/icvts/ivw065
Long-term echocardiographic follow-up of untreated 2+ functional tricuspid regurgitation in patients undergoing mitral valve surgery
Abstract
Objectives: Concomitant tricuspid valve surgery with mitral valve surgery is recommended for patients with severe functional tricuspid regurgitation (TR). However, the treatment for 2+ TR (mild TR) remains controversial. Here, we evaluated the long-term results of untreated 2+ TR in patients undergoing mitral valve surgery.
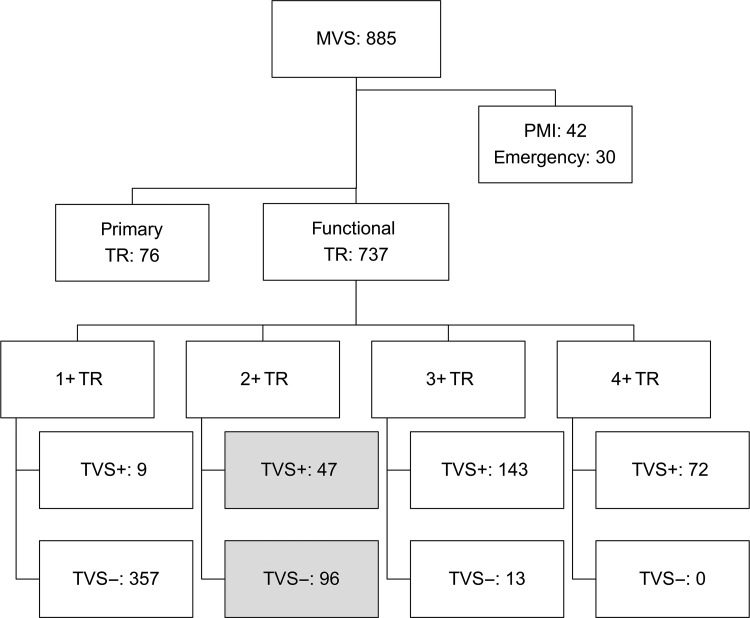
Methods: We retrospectively reviewed the records of 96 patients with untreated 2+ TR among 885 patients who underwent mitral valve surgery from 2003 to 2010. Exclusion criteria were tricuspid valve surgery (TVS), emergency surgery, primary TR and pacemaker lead through the tricuspid valve. We assessed survival and freedom from heart failure. The freedom from 3+ (moderate) or 4+ (severe) TR was investigated by echocardiographic data at pre- and postoperative week 1, then at 1, 3, 5, 7 and 10 postoperative years, which were compared with those in patients who had 2+ TR preoperatively and underwent concomitant TVS in the same period (n = 47).
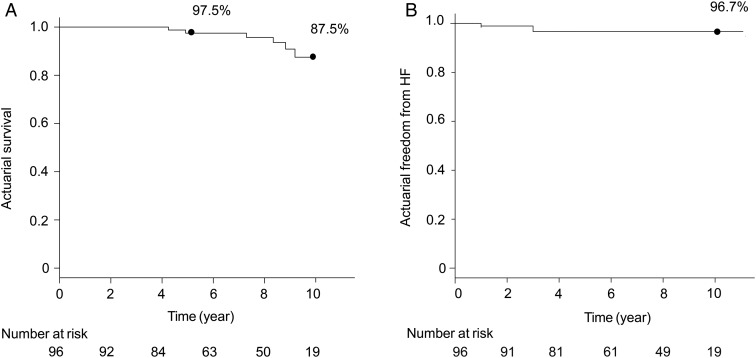
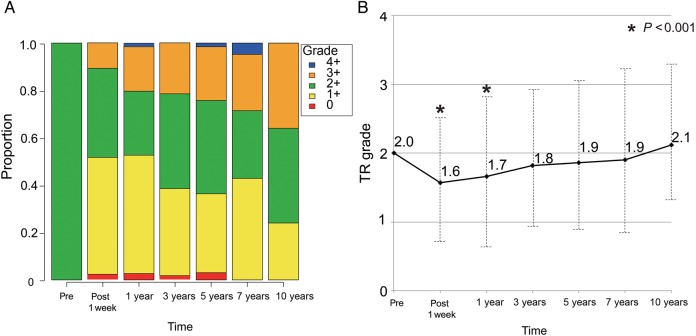
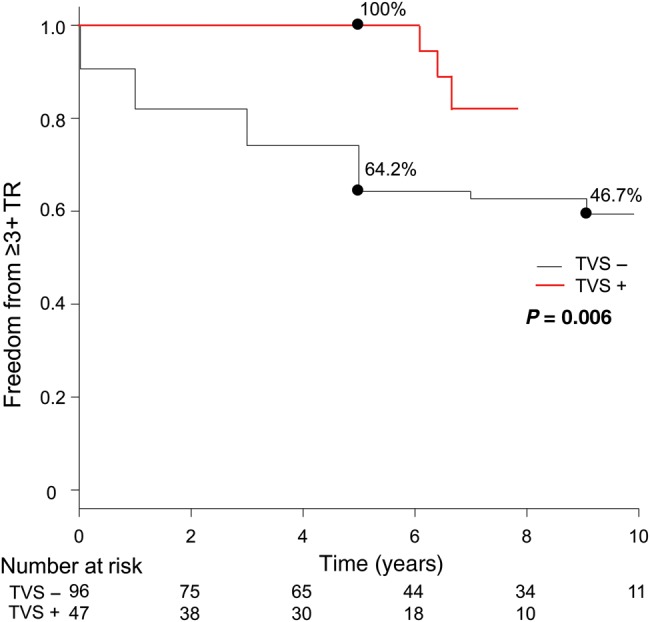
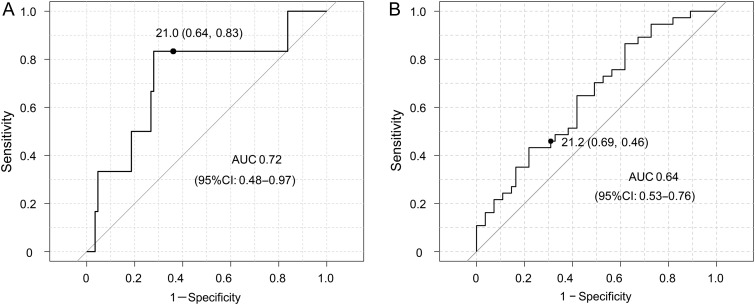
Results: The mean follow-up was 7.1 ± 2.7 years. There was no 30-day mortality. The survival rate was 97.5% at 5 years and 87.5% at 10 years. The independent risk factors for mortality were age (OR 1.2, P = 0.03) and left ventricular ejection fraction (OR 0.9, P = 0.03). Untreated 2+ TR improved transiently within the first postoperative year (P < 0.001), but progressed again in the mid- to long term. Freedom from ≥3+ TR was 64.2% at 5 years and 46.7% at 10 years, which was significantly lower than that from ≥3+ TR in patients who underwent concomitant TVS (P = 0.006). The independent risk factors for TR progression (≥3 + TR) were age (OR 1.1, P = 0.005), atrial fibrillation (OR 2.2, P = 0.04) and tricuspid annular diameter (TAD) index (mm/m(2); OR 1.1, P = 0.02). Receiver operating characteristic curves showed that the optimal TAD index cut-off value was 21.0 for long-term survival [area under the curve (AUC) = 0.72] and 21.2 for TR progression (AUC = 0.64).
Conclusions: Although untreated, 2+ TR significantly improved after mitral valve surgery, it then progressed again in the mid- to long term. Therefore, concomitant TVS should be considered in patients with 2+ TR who have dilated tricuspid annulus or atrial fibrillation, if feasible.
Keywords: Atrial fibrillation; Long term; Mitral valve surgery; Tricuspid annular diameter; Tricuspid regurgitation.
© The Author 2016. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
Comment in
-
eComment. Echocardiographic variables which may influence the long-term results of tricuspid valve surgery.Interact Cardiovasc Thorac Surg. 2016 Jul;23(1):102-3. doi: 10.1093/icvts/ivw118. Interact Cardiovasc Thorac Surg. 2016. PMID: 27325656 Free PMC article. No abstract available.
References
-
- Shiran A, Sagie A. Tricuspid regurgitation in mitral valve disease incidence, prognostic implications, mechanism, and management. J Am Coll Cardiol 2009;53:401–18. - PubMed
-
- Fukuda S, Gillinov AM, Song JM, Daimon M, Kongsaerepong V, Thomas JD et al. . Echocardiographic insights into atrial and ventricular mechanisms of functional tricuspid regurgitation. Am Heart J 2006;152:1208–14. - PubMed
-
- Fukuda S, Gillinov AM, McCarthy PM, Stewart WJ, Song JM, Kihara T et al. . Determinants of recurrent or residual functional tricuspid regurgitation after tricuspid annuloplasty. Circulation 2006;114:I-582–7. - PubMed
-
- Braunwald NS, Ross J, Morrow AG. Conservative management of tricuspid regurgitation in patients undergoing mitral valve replacement. Circulation 1967;35:I-63–9. - PubMed
-
- Duran CM, Pomar JL, Colman T, Figueroa A, Revuelta JM, Ubago JL. Is tricuspid valve repair necessary? J Thorac Cardiovasc Surg 1980;80:849–60. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
