

Association between Zika virus and microcephaly in French Polynesia, 2013-15: a retrospective study
- PMID: 26993883
- PMCID: PMC4909533
- DOI: 10.1016/S0140-6736(16)00651-6
Association between Zika virus and microcephaly in French Polynesia, 2013-15: a retrospective study
Abstract
Background: The emergence of Zika virus in the Americas has coincided with increased reports of babies born with microcephaly. On Feb 1, 2016, WHO declared the suspected link between Zika virus and microcephaly to be a Public Health Emergency of International Concern. This association, however, has not been precisely quantified.
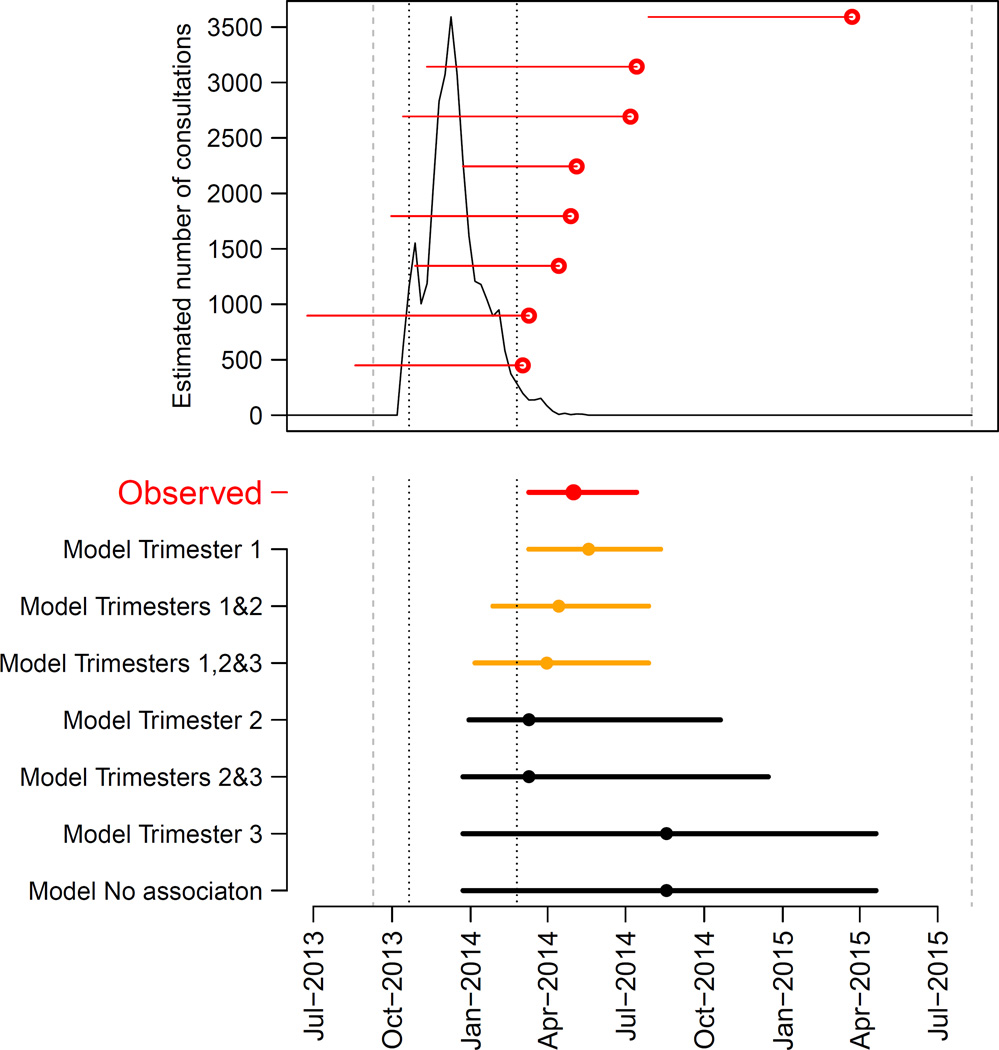
Methods: We retrospectively analysed data from a Zika virus outbreak in French Polynesia, which was the largest documented outbreak before that in the Americas. We used serological and surveillance data to estimate the probability of infection with Zika virus for each week of the epidemic and searched medical records to identify all cases of microcephaly from September, 2013, to July, 2015. Simple models were used to assess periods of risk in pregnancy when Zika virus might increase the risk of microcephaly and estimate the associated risk.
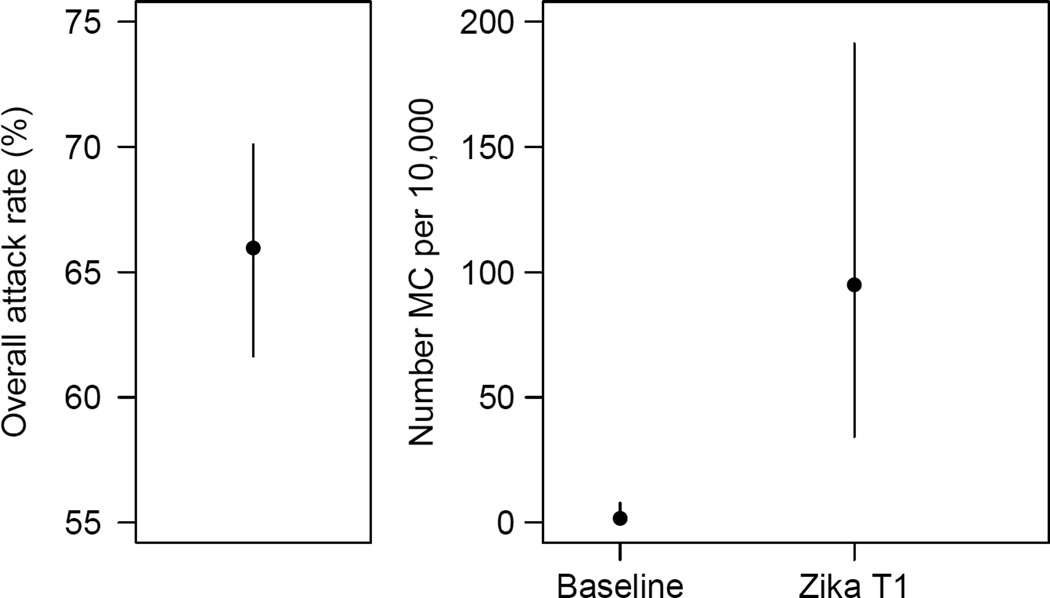
Findings: The Zika virus outbreak began in October, 2013, and ended in April, 2014, and 66% (95% CI 62-70) of the general population were infected. Of the eight microcephaly cases identified during the 23-month study period, seven (88%) occurred in the 4-month period March 1 to July 10, 2014. The timing of these cases was best explained by a period of risk in the first trimester of pregnancy. In this model, the baseline prevalence of microcephaly was two cases (95% CI 0-8) per 10,000 neonates, and the risk of microcephaly associated with Zika virus infection was 95 cases (34-191) per 10,000 women infected in the first trimester. We could not rule out an increased risk of microcephaly from infection in other trimesters, but models that excluded the first trimester were not supported by the data.
Interpretation: Our findings provide a quantitative estimate of the risk of microcephaly in fetuses and neonates whose mothers are infected with Zika virus.
Funding: Labex-IBEID, NIH-MIDAS, AXA Research fund, EU-PREDEMICS.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures
Comment in
-
Microcephaly and Zika virus infection.Lancet. 2016 May 21;387(10033):2070-2072. doi: 10.1016/S0140-6736(16)00742-X. Epub 2016 Mar 16. Lancet. 2016. PMID: 26993880 No abstract available.
-
Could clinical symptoms be a predictor of complications in Zika virus infection?Lancet. 2016 Jul 23;388(10042):338. doi: 10.1016/S0140-6736(16)31104-7. Lancet. 2016. PMID: 27477156 No abstract available.
-
Could clinical symptoms be a predictor of complications in Zika virus infection? - Authors' reply.Lancet. 2016 Jul 23;388(10042):338-339. doi: 10.1016/S0140-6736(16)31017-0. Lancet. 2016. PMID: 27477157 No abstract available.
Similar articles
-
Congenital cerebral malformations and dysfunction in fetuses and newborns following the 2013 to 2014 Zika virus epidemic in French Polynesia.Euro Surveill. 2016;21(13). doi: 10.2807/1560-7917.ES.2016.21.13.30181. Euro Surveill. 2016. PMID: 27063794
-
Infection-related microcephaly after the 2015 and 2016 Zika virus outbreaks in Brazil: a surveillance-based analysis.Lancet. 2017 Aug 26;390(10097):861-870. doi: 10.1016/S0140-6736(17)31368-5. Epub 2017 Jun 21. Lancet. 2017. PMID: 28647172
-
Association and birth prevalence of microcephaly attributable to Zika virus infection among infants in Paraíba, Brazil, in 2015-16: a case-control study.Lancet Child Adolesc Health. 2018 Mar;2(3):205-213. doi: 10.1016/S2352-4642(18)30020-8. Epub 2018 Jan 12. Lancet Child Adolesc Health. 2018. PMID: 30169255
-
Zika Virus in the Americas: A Review for Clinicians.Mayo Clin Proc. 2016 Apr;91(4):514-21. doi: 10.1016/j.mayocp.2016.02.017. Mayo Clin Proc. 2016. PMID: 27046524 Review.
-
An update on Zika virus infection.Lancet. 2017 Nov 4;390(10107):2099-2109. doi: 10.1016/S0140-6736(17)31450-2. Epub 2017 Jun 21. Lancet. 2017. PMID: 28647173 Review.
Cited by
-
Characterization of a Zika Virus Isolate from Colombia.PLoS Negl Trop Dis. 2016 Sep 21;10(9):e0005019. doi: 10.1371/journal.pntd.0005019. eCollection 2016 Sep. PLoS Negl Trop Dis. 2016. PMID: 27654889 Free PMC article.
-
A Zika virus protein expression screen in Drosophila to investigate targeted host pathways during development.Dis Model Mech. 2024 Feb 1;17(2):dmm050297. doi: 10.1242/dmm.050297. Epub 2024 Feb 28. Dis Model Mech. 2024. PMID: 38214058 Free PMC article.
-
The Brazilian Zika virus strain causes birth defects in experimental models.Nature. 2016 Jun 9;534(7606):267-71. doi: 10.1038/nature18296. Epub 2016 May 11. Nature. 2016. PMID: 27279226 Free PMC article.
-
Contributions of Immune Response to Individual Differences in Zika Virus Infection.Ann Public Health Res. 2017;4(2):1060. Epub 2017 Apr 5. Ann Public Health Res. 2017. PMID: 36468937 Free PMC article.
-
A Comprehensive Systems Biology Approach to Studying Zika Virus.PLoS One. 2016 Sep 1;11(9):e0161355. doi: 10.1371/journal.pone.0161355. eCollection 2016. PLoS One. 2016. PMID: 27584813 Free PMC article.
References
-
- Gubler D, Kuno GLM. Flaviviruses. In: Knipe DMHP, Griffin DE, Lamb RA, Martin MA, et al., editors. Fields virology. Philadelphia, PA: Lippincott Williams & Wilkins Publishers; 2007. pp. 1153–1252.
-
- WHO. Zika situation report. [Last accessed on 27 Feb 2016];2016 Feb 19; Available at http://www.who.int/emergencies/zika-virus/situation-report/19-february-2...
-
- WHO. Guillain-Barré syndrome - El Salvador. [Last accessed on Feb 5 2016];2016 Jan 21; Available at http://www.who.int/csr/don/21-january-2016-gbs-el-salvador/en/
-
- ECDC. Risk assessment: Zika virus epidemic in the Americas: potentially associated with microcephaly and Guillain-Barré syndrome. [Last accessed on 5 Feb 2016];2016 Available at.
-
- Soares de Araujo J, Regis T, Gomes R, et al. Microcephaly in northeast Brasil: a review of 16 208 births between 2012 and 2015. [Last accessed on 8 Feb 2015];Bull World Health Organ. 2016 Available at http://who.int/bulletin/online_first/16-170639.pdf?ua=1 [Submitted]
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
