

Relationship Between the Duration of Cardiopulmonary Resuscitation and Favorable Neurological Outcomes After Out-of-Hospital Cardiac Arrest: A Prospective, Nationwide, Population-Based Cohort Study
- PMID: 26994129
- PMCID: PMC4943259
- DOI: 10.1161/JAHA.115.002819
Relationship Between the Duration of Cardiopulmonary Resuscitation and Favorable Neurological Outcomes After Out-of-Hospital Cardiac Arrest: A Prospective, Nationwide, Population-Based Cohort Study
Abstract
Background: The determination of appropriate duration of in-the-field cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest (OHCA) patients is one of the biggest challenges for emergency medical service providers and clinicians. The appropriate CPR duration before termination of resuscitation remains unclear and may differ based on initial rhythm. We aimed to determine the relationship between CPR duration and post-OHCA outcomes.
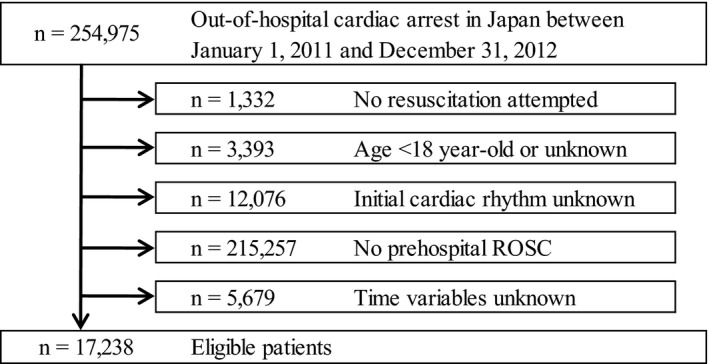
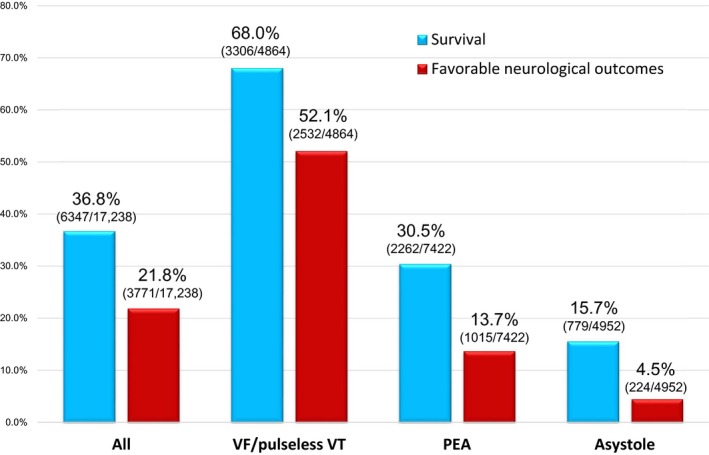
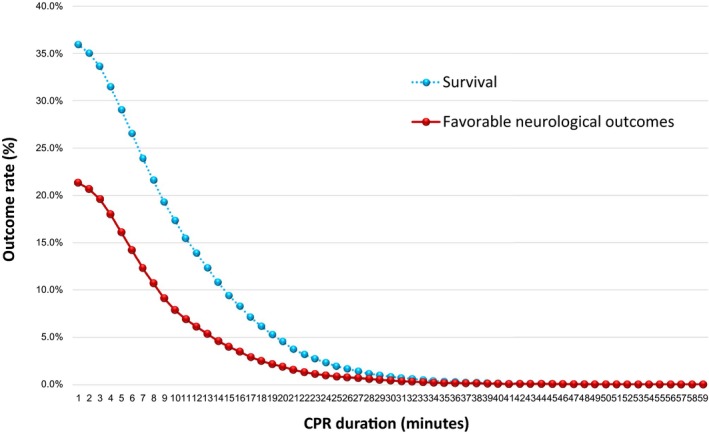
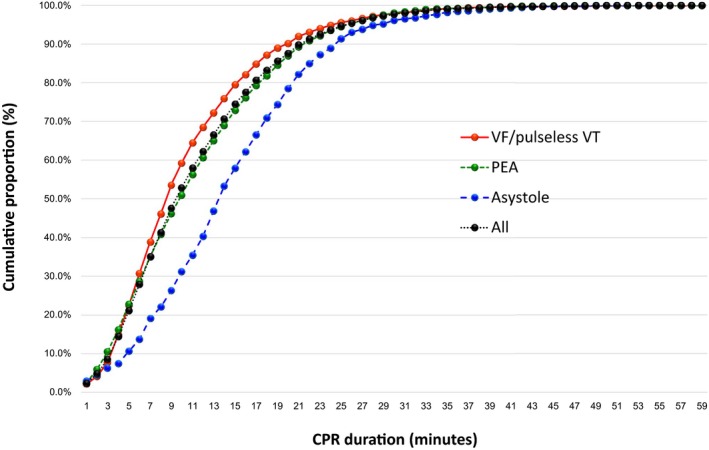
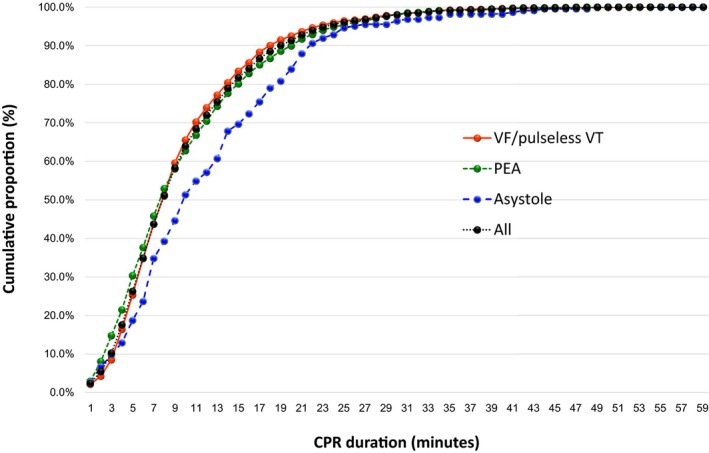
Methods and results: We analyzed the records of 17 238 OHCA patients (age ≥18 years) who achieved prehospital return of spontaneous circulation. Data were prospectively recorded in a nationwide, Japanese database between 2011 and 2012. The time from CPR initiation to prehospital return of spontaneous circulation (CPR duration) was calculated. The primary end point was 1-month survival with favorable neurological outcomes (Cerebral Performance Category [CPC] scale; CPC 1-2). The 1-month CPC 1-2 rate was 21.8% (n=3771). CPR duration was inversely associated with 1-month CPC 1-2 (adjusted unit odds ratio: 0.95, 95% CI: 0.94-0.95). Among all patients, a cumulative proportion of >99% of 1-month CPC 1-2 was achieved with a CPR duration of 35 minutes. When sorted by the initial rhythm, the CPR duration producing more than 99% of survivors with CPC 1-2 was 35 minutes for shockable rhythms and pulseless electrical activity, and 42 minutes for asystole.
Conclusions: CPR duration was independently and inversely associated with favorable 1-month neurological outcomes. The critical prehospital CPR duration for OHCA was 35 minutes in patients with initial shockable rhythms and pulseless electrical activity, and 42 minutes in those with initial asystole.
Keywords: cardiopulmonary resuscitation; epidemiology; heart arrest; resuscitation.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Ro YS, Shin SD, Kitamura T, Lee EJ, Kajino K, Song KJ, Nishiyama C, Kong SY, Sakai T, Nishiuchi T, Hayashi Y, Iwami T; Seoul‐Osaka Resuscitation Study Group . Temporal trends in out‐of‐hospital cardiac arrest survival outcomes between two metropolitan communities: Seoul‐Osaka resuscitation study. BMJ Open. 2015;5:e007626. - PMC - PubMed
-
- Wong MK, Morrison LJ, Qiu F, Austin PC, Cheskes S, Dorian P, Scales DC, Tu JV, Verbeek PR, Wijeysundera HC, Ko DT. Trends in short‐ and long‐term survival among out‐of‐hospital cardiac arrest patients alive at hospital arrival. Circulation. 2014;130:1883–1890. - PubMed
-
- Kitamura T, Iwami T, Kawamura T, Nitta M, Nagao K, Nonogi H, Yonemoto N, Kimura T; for the Japanese Circulation Society Resuscitation Science Study Group . Nationwide improvements in survival from out‐of‐hospital cardiac arrest in Japan. Circulation. 2012;126:2834–2843. - PubMed
-
- Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, Chen WJ, Huang SC, Chi NH, Wang CH, Chen LC, Tsai PR, Wang SS, Hwang JJ, Lin FY. Cardiopulmonary resuscitation with assisted extracorporeal life‐support versus conventional cardiopulmonary resuscitation in adults with in‐hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008;372:554–561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
