

Meta-analysis of negative-pressure wound therapy for closed surgical incisions
- PMID: 26994715
- PMCID: PMC5069647
- DOI: 10.1002/bjs.10084
Meta-analysis of negative-pressure wound therapy for closed surgical incisions
Abstract
Background: Postoperative wound complications are common following surgical procedures. Negative-pressure wound therapy (NPWT) is well recognized for the management of open wounds and has been applied recently to closed surgical incisions. The evidence base to support this intervention is limited. The aim of this study was to assess whether NPWT reduces postoperative wound complications when applied to closed surgical incisions.
Methods: This was a systematic review and meta-analysis of randomized clinical trials of NPWT compared with standard postoperative dressings on closed surgical incisions.
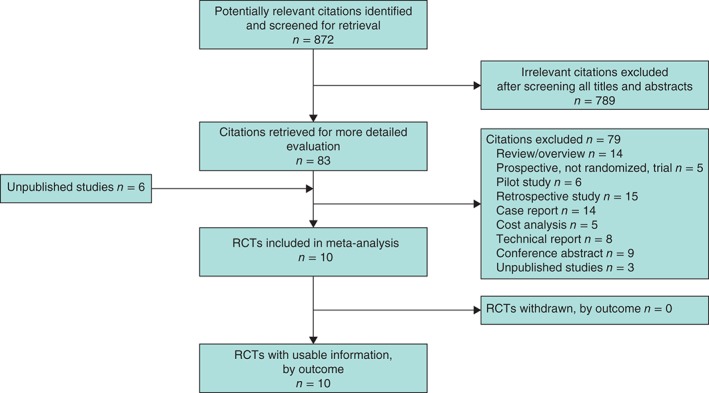
Results: Ten studies met the inclusion criteria, reporting on 1311 incisions in 1089 patients. NPWT was associated with a significant reduction in wound infection (relative risk (RR) 0·54, 95 per cent c.i. 0·33 to 0·89) and seroma formation (RR 0·48, 0·27 to 0·84) compared with standard care. The reduction in wound dehiscence was not significant. The numbers needed to treat were three (seroma), 17 (dehiscence) and 25 (infection). Methodological heterogeneity across studies led to downgrading of the quality of evidence to moderate for infection and seroma, and low for dehiscence.
Conclusion: Compared with standard postoperative dressings, NPWT significantly reduced the rate of wound infection and seroma when applied to closed surgical wounds. Heterogeneity between the included studies means that no general recommendations can be made yet.
© 2016 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures

References
-
- Culver DH, Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG et al Surgical wound infection rates by wound class, operative procedure, and patient risk index. National Nosocomial Infections Surveillance System. Am J Med 1991; 91: 152S–157S. - PubMed
-
- Haley RW, Culver DH, Morgan WM, White JW, Emori TG, Hooton TM. Identifying patients at high risk of surgical wound infection. A simple multivariate index of patient susceptibility and wound contamination. Am J Epidemiol 1985; 121: 206–215. - PubMed
-
- Leth RA, Uldbjerg N, Norgaard M, Moller JK, Thomsen RW. Obesity, diabetes, and the risk of infections diagnosed in hospital and post‐discharge infections after cesarean section: a prospective cohort study. Acta Obstet Gynecol Scand 2011; 90: 501–509. - PubMed
-
- Riou JP, Cohen JR, Johnson H Jr . Factors influencing wound dehiscence. Am J Surg 1992; 163: 324–330. - PubMed
-
- Wilson JA, Clark JJ. Obesity: impediment to postsurgical wound healing. Adv Skin Wound Care 2004; 17: 426–435. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
