

Adaptive immunity in the liver
- PMID: 26996069
- PMCID: PMC4856810
- DOI: 10.1038/cmi.2016.4
Adaptive immunity in the liver
Abstract
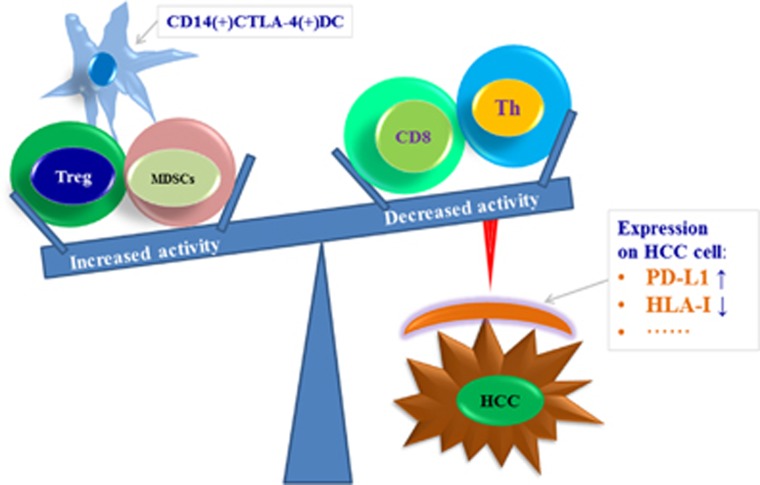
The anatomical architecture of the human liver and the diversity of its immune components endow the liver with its physiological function of immune competence. Adaptive immunity is a major arm of the immune system that is organized in a highly specialized and systematic manner, thus providing long-lasting protection with immunological memory. Adaptive immunity consists of humoral immunity and cellular immunity. Cellular immunity is known to have a crucial role in controlling infection, cancer and autoimmune disorders in the liver. In this article, we will focus on hepatic virus infections, hepatocellular carcinoma and autoimmune disorders as examples to illustrate the current understanding of the contribution of T cells to cellular immunity in these maladies. Cellular immune suppression is primarily responsible for chronic viral infections and cancer. However, an uncontrolled auto-reactive immune response accounts for autoimmunity. Consequently, these immune abnormalities are ascribed to the quantitative and functional changes in adaptive immune cells and their subsets, innate immunocytes, chemokines, cytokines and various surface receptors on immune cells. A greater understanding of the complex orchestration of the hepatic adaptive immune regulators during homeostasis and immune competence are much needed to identify relevant targets for clinical intervention to treat immunological disorders in the liver.
Figures


References
-
- Doherty DG. Immunity, tolerance and autoimmunity in the liver: a comprehensive review. J Autoimmun 2015; 66: 60–75. - PubMed
-
- Xu X, Zhang S, Jin R, Wang K, Li P, Lin L et al. Retention and tolerance of autoreactive CD4(+) recent thymic emigrants in the liver. J Autoimmun 2015; 56: 87–97. - PubMed
-
- Zhang H, Liu Y, Bian Z, Huang S, Han X, You Z et al. The critical role of myeloid-derived suppressor cells and FXR activation in immune-mediated liver injury. J Autoimmun 2014; 53: 55–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
