

An ectopic renin-secreting adrenal corticoadenoma in a child with malignant hypertension
- PMID: 26997629
- PMCID: PMC4823597
- DOI: 10.14814/phy2.12728
An ectopic renin-secreting adrenal corticoadenoma in a child with malignant hypertension
Abstract
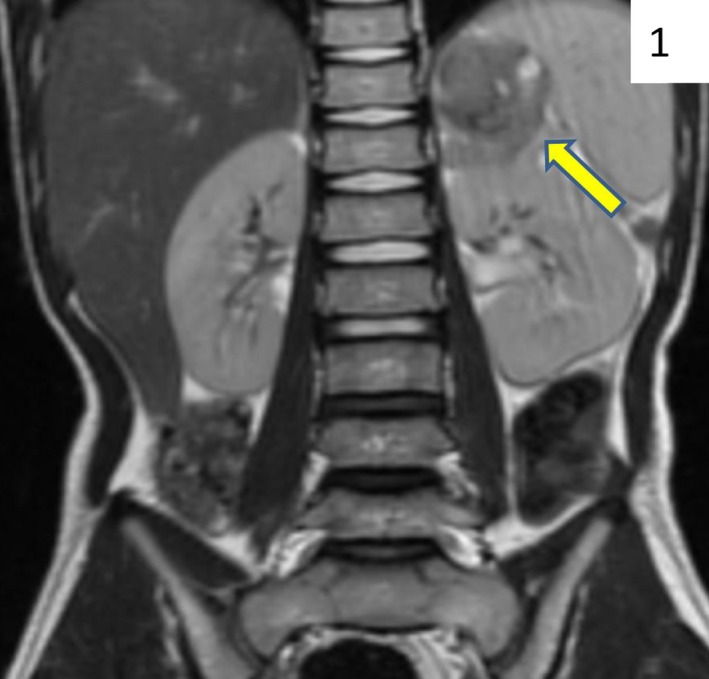
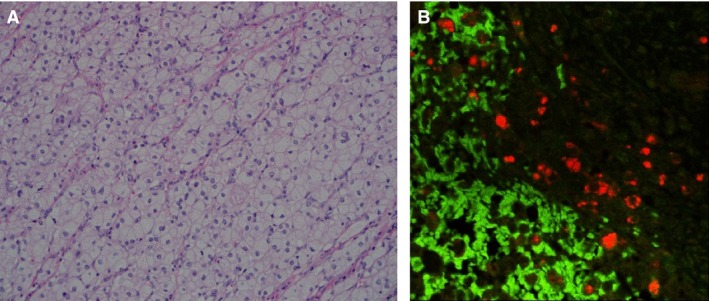
A previously healthy 7-year-old male presented with hypertensive emergency, hypokalemia, and elevated plasma renin activity and aldosterone levels. There was no evidence of virilization or cushingoid features. MRI of the abdomen revealed a large (5 × 5 × 3 cm) peripherally enhancing, heterogeneous mass arising from the left adrenal gland. The patient was treated for a suspected pheochromocytoma. However, his blood pressure was not responsive to alpha-blockade. Blood pressure was controlled with a calcium channel blocker and an angiotensin-converting enzyme (ACE) inhibitor. A complete surgical resection of the mass was performed. Postoperatively, his blood pressure normalized and he did not require antihypertensives. On pathological examination, the tumor tissue stained negative for chromogranin and positive for renin. The final diagnosis was renin-secreting adrenal corticoadenoma, an extremely rare adrenal tumor not previously reported in a pediatric patient. Malignant hypertension due to a renin-secreting tumor may need to be distinguished from a pheochromocytoma if alpha-adrenergic blockade is ineffective.
Keywords: Adrenal mass; aldosterone; ectopic renin; malignant hypertension; pheochromocytoma.
© 2016 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of the American Physiological Society and The Physiological Society.
Figures
Similar articles
-
Ectopic Adrenocortical Adenoma Causing Malignant Hypertension and Hypokalemia.Am J Case Rep. 2025 Jul 24;26:e948022. doi: 10.12659/AJCR.948022. Am J Case Rep. 2025. PMID: 40702712 Free PMC article.
-
Malignant hypertension secondary to cortisol-secreting adrenal tumour.N Z Med J. 2005 Jun 3;118(1216):U1498. N Z Med J. 2005. PMID: 15937532
-
[Tetraparesis revealing Conn adenoma in a pregnant woman].Pan Afr Med J. 2016 Sep 27;25:24. doi: 10.11604/pamj.2016.25.24.8245. eCollection 2016. Pan Afr Med J. 2016. PMID: 28154716 Free PMC article. French.
-
Aldosterone-secreting adrenal cortical adenoma in an 11-year-old child and collective review of the literature.Eur J Pediatr. 1994 Oct;153(10):715-7. doi: 10.1007/BF01954485. Eur J Pediatr. 1994. PMID: 7813526 Review.
-
A case of normoreninemic aldosterone-producing adenoma associated with chronic renal failure: case report and literature review.Endocrine. 2003 Aug;21(3):221-6. doi: 10.1385/ENDO:21:3:221. Endocrine. 2003. PMID: 14515005 Review.
Cited by
-
Malignant Pheochromocytomas/Paragangliomas and Ectopic Hormonal Secretion: A Case Series and Review of the Literature.Cancers (Basel). 2019 May 24;11(5):724. doi: 10.3390/cancers11050724. Cancers (Basel). 2019. PMID: 31137729 Free PMC article. Review.
References
-
- Bader, M. , and Ganten D.. 2008. Update on tissue renin‐angiotensin systems. J. Mol. Med. (Berl) 86:615–621. - PubMed
-
- Boyle, J. G. , Davidson D. F., Perry C. G., and Connell J. M.. 2007. Comparison of diagnostic accuracy of urinary free metanephrines, vanillyl mandelic Acid, and catecholamines and plasma catecholamines for diagnosis of pheochromocytoma. J. Clin. Endocrinol. Metab. 92:4602–4608. - PubMed
-
- Corvol, P. , Pinet F., Plouin P. F., Bruneval P., and Menard J.. 1994. Renin‐secreting tumors. Endocrinol. Metab. Clin. North Am. 23:255–270. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
