

Effects of combination PPARγ agonist and angiotensin receptor blocker on glomerulosclerosis
- PMID: 26999660
- PMCID: PMC6117161
- DOI: 10.1038/labinvest.2016.42
Effects of combination PPARγ agonist and angiotensin receptor blocker on glomerulosclerosis
Abstract
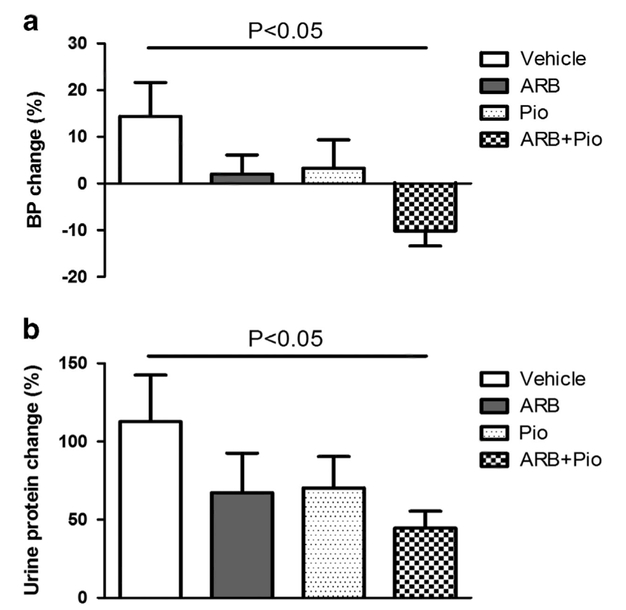
We previously observed that high-dose angiotensin receptor blocker (ARB) can induce regression of existing glomerulosclerosis. We also found that proliferator-activated recepto-γ (PPARγ) agonist can attenuate glomerulosclerosis in a nondiabetic model of kidney disease, with specific protection of podocytes. We now assessed effects of combination therapy with ARB and pioglitazone on established glomerulosclerosis. Sprague-Dawley male rats underwent 5/6 nephrectomy (5/6 Nx) at week 0 and renal biopsy at week 8. Rats were randomized to groups with equal starting moderate glomerulosclerosis, and treated with ARB, PPARγ agonist (pioglitazone), combination or vehicle from weeks 8 to 12. Body weight, systolic blood pressure (SBP), and urinary protein (UP) were measured at intervals. In rats with established sclerosis, SBP, UP, and GS were equal in all groups at week 8 before treatment by study design. Untreated control rats had hypertension, decreased GFR, and progressive proteinuria and glomerulosclerosis at week 12. Only combination therapy significantly ameliorated hypertension and proteinuria. ARB alone or pioglitazone alone had only numerically lower SBP and UP than vehicle at week 12. Both pioglitazone alone and combination had significantly less decline in GFR than vehicle. Combination-induced regression of glomerulosclerosis in more rats from weeks 8 to 12 than ARB or pioglitazone alone. In parallel, combination treatment reduced plasminogen activator inhibitor-1 expression and macrophage infiltration, and preserved podocytes compared with vehicle. These results were linked to increased AT2 receptor and Mas1 mRNA in the combination group. PPARγ agonists in combination with ARB augment regression of glomerulosclerosis, with downregulation of injurious RAAS components vs PPARγ alone, with increased anti-fibrotic/healing RAAS components, enhanced podocyte preservation, and decreased inflammation and profibrotic mechanisms.
Conflict of interest statement
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Figures





References
-
- Eddy AA, Fogo AB. Plasminogen activator inhibitor-1 in chronic kidney disease: evidence and mechanisms of action. J Am Soc Nephrol 2006;17:2999–3012. - PubMed
-
- Oparil S, Silfani TN, Walker JF. Role of angiotensin receptor blockers as monotherapy in reaching blood pressure goals. Am J Hypertens 2005;18:287–294. - PubMed
-
- Yusuf S, Teo KK, Pogue J et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008;358:1547–1559. - PubMed
-
- Albertazzi V, Yang H-C, Ma L-J et al. Sustained regression and improved survival with high dose ARB in 5/6 nephrectomy rats. J Am Soc Nephrol 2008;19:193A.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
