

Randomized, Blinded Pilot Testing of Nonconventional Stimulation Patterns and Shapes in Parkinson's Disease and Essential Tremor: Evidence for Further Evaluating Narrow and Biphasic Pulses
- PMID: 27000764
- PMCID: PMC4914444
- DOI: 10.1111/ner.12397
Randomized, Blinded Pilot Testing of Nonconventional Stimulation Patterns and Shapes in Parkinson's Disease and Essential Tremor: Evidence for Further Evaluating Narrow and Biphasic Pulses
Abstract
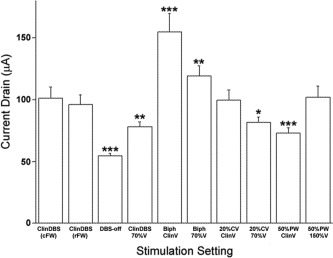
Objectives: Evidence suggests that nonconventional programming may improve deep brain stimulation (DBS) therapy for movement disorders. The primary objective was to assess feasibility of testing the tolerability of several nonconventional settings in Parkinson's disease (PD) and essential tremor (ET) subjects in a single office visit. Secondary objectives were to explore for potential efficacy signals and to assess the energy demand on the implantable pulse-generators (IPGs).
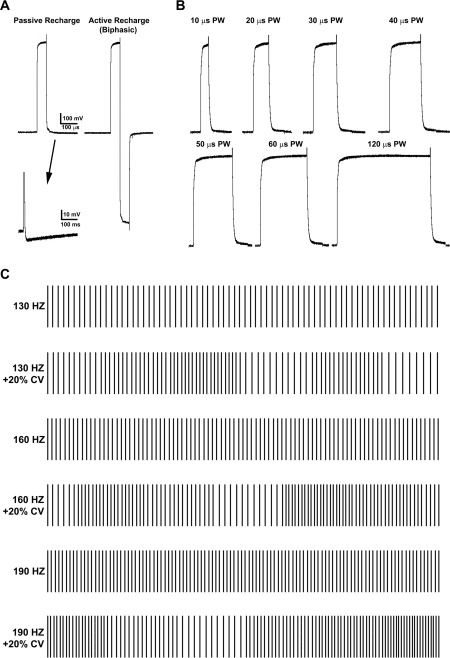
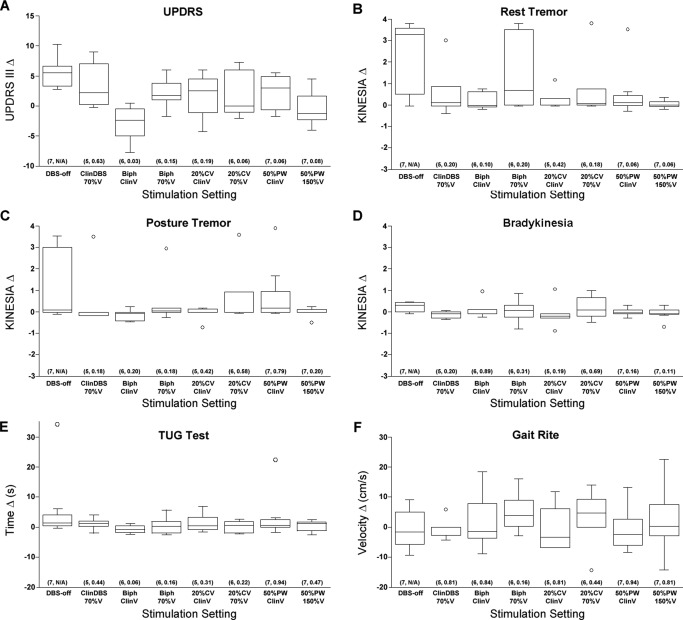
Materials and methods: A custom firmware (FW) application was developed and acutely uploaded to the IPGs of eight PD and three ET subjects, allowing delivery of several nonconventional DBS settings, including narrow pulse widths, square biphasic pulses, and irregular pulse patterns. Standard clinical rating scales and several objective measures were used to compare motor outcomes with sham, clinically-optimal and nonconventional settings. Blinded and randomized testing was conducted in a traditional office setting.
Results: Overall, the nonconventional settings were well tolerated. Under these conditions it was also possible to detect clinically-relevant differences in DBS responses using clinical rating scales but not objective measures. Compared to the clinically-optimal settings, some nonconventional settings appeared to offer similar benefit (e.g., narrow pulse widths) and others lesser benefit. Moreover, the results suggest that square biphasic pulses may deliver greater benefit. No unexpected IPG efficiency disadvantages were associated with delivering nonconventional settings.
Conclusions: It is feasible to acutely screen nonconventional DBS settings using controlled study designs in traditional office settings. Simple IPG FW upgrades may provide more DBS programming options for optimizing therapy. Potential advantages of narrow and biphasic pulses deserve follow up.
Keywords: Biphasic pulses; Parkinson's disease; deep brain stimulation; essential tremor; irregular patterns; narrow pulse width.
© 2016 The Authors. Neuromodulation: Technology at the Neural Interface published by Wiley Periodicals, Inc. on behalf of International Neuromodulation Society.
Figures
References
-
- Deep‐Brain Stimulation for Parkinson's Disease Study Group. Deep‐brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson's disease. N Engl J Med 2001;345:956–963. - PubMed
-
- Koller WC, KE Lyons, SB Wilkinson et al. Long‐term safety and efficacy of unilateral deep brain stimulation of the thalamus in essential tremor. Mov Disord 2001;16:464–468. - PubMed
-
- Vercueil L, P Pollak, V Fraix et al. Deep brain stimulation in the treatment of severe dystonia. J Neurol 2001;248:695–700. - PubMed
-
- Moro E, RJ Esselink, J Xie et al. The impact on Parkinson's disease of electrical parameter settings in STN stimulation. Neurology 2002;59:706–713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
