

Steroid Sulfatase Deficiency and Androgen Activation Before and After Puberty
- PMID: 27003302
- PMCID: PMC4891801
- DOI: 10.1210/jc.2015-4101
Steroid Sulfatase Deficiency and Androgen Activation Before and After Puberty
Abstract
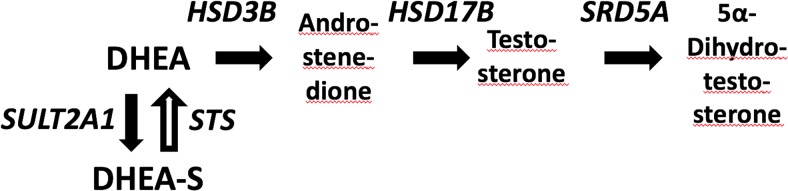
Context: Steroid sulfatase (STS) cleaves the sulfate moiety off steroid sulfates, including dehydroepiandrosterone (DHEA) sulfate (DHEAS), the inactive sulfate ester of the adrenal androgen precursor DHEA. Deficient DHEA sulfation, the opposite enzymatic reaction to that catalyzed by STS, results in androgen excess by increased conversion of DHEA to active androgens. STS deficiency (STSD) due to deletions or inactivating mutations in the X-linked STS gene manifests with ichthyosis, but androgen synthesis and metabolism in STSD have not been studied in detail yet.
Patients and methods: We carried out a cross-sectional study in 30 males with STSD (age 6-27 y; 13 prepubertal, 5 peripubertal, and 12 postpubertal) and 38 age-, sex-, and Tanner stage-matched healthy controls. Serum and 24-hour urine steroid metabolome analysis was performed by mass spectrometry and genetic analysis of the STS gene by multiplex ligation-dependent probe amplification and Sanger sequencing.
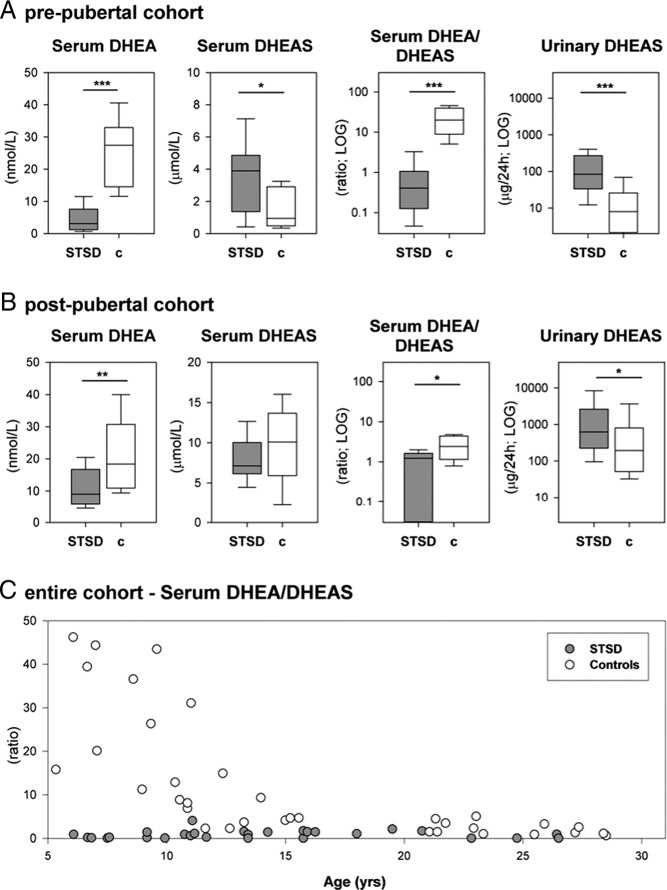
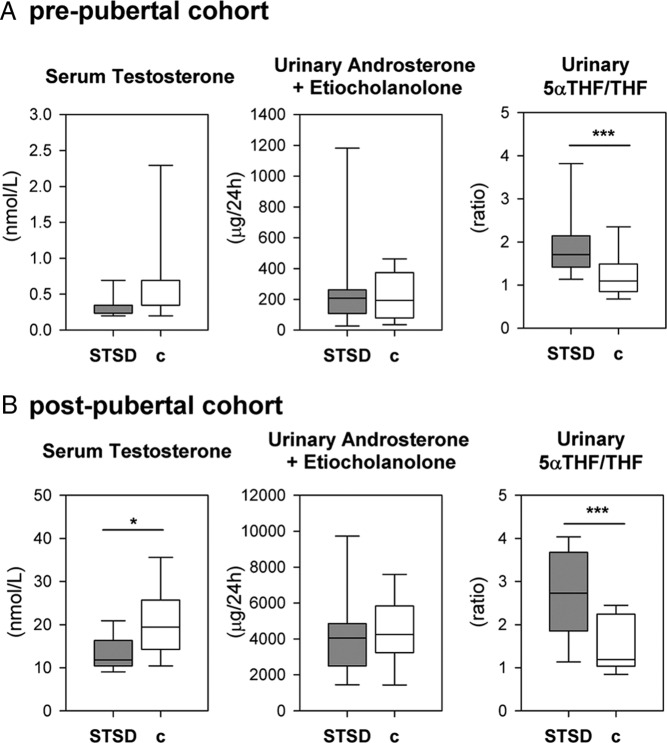
Results: Genetic analysis showed STS mutations in all patients, comprising 27 complete gene deletions, 1 intragenic deletion and 2 missense mutations. STSD patients had apparently normal pubertal development. Serum and 24-hour urinary DHEAS were increased in STSD, whereas serum DHEA and testosterone were decreased. However, total 24-hour urinary androgen excretion was similar to controls, with evidence of increased 5α-reductase activity in STSD. Prepubertal healthy controls showed a marked increase in the serum DHEA to DHEAS ratio that was absent in postpubertal controls and in STSD patients of any pubertal stage.
Conclusions: In STSD patients, an increased 5α-reductase activity appears to compensate for a reduced rate of androgen generation by enhancing peripheral androgen activation in affected patients. In healthy controls, we discovered a prepubertal surge in the serum DHEA to DHEAS ratio that was absent in STSD, indicative of physiologically up-regulated STS activity before puberty. This may represent a fine tuning mechanism for tissue-specific androgen activation preparing for the major changes in androgen production during puberty.
Figures
References
-
- Noordam C, Dhir V, McNelis JC, et al. Inactivating PAPSS2 mutations in a patient with premature pubarche. N Engl J Med. 2009;360(22):2310–2318. - PubMed
-
- Reed MJ, Purohit A, Woo LW, Newman SP, Potter BV. Steroid sulfatase: molecular biology, regulation, and inhibition. Endocr Rev. 2005;26(2):171–202. - PubMed
-
- Hammer F, Subtil S, Lux P, et al. No evidence for hepatic conversion of dehydroepiandrosterone (DHEA) sulfate to DHEA: in vivo and in vitro studies. J Clin Endocrinol Metab. 2005;90(6):3600–3605. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
