

Fracture Prediction With Modified-FRAX in Older HIV-Infected and Uninfected Men
- PMID: 27003493
- PMCID: PMC4942335
- DOI: 10.1097/QAI.0000000000000998
Fracture Prediction With Modified-FRAX in Older HIV-Infected and Uninfected Men
Abstract
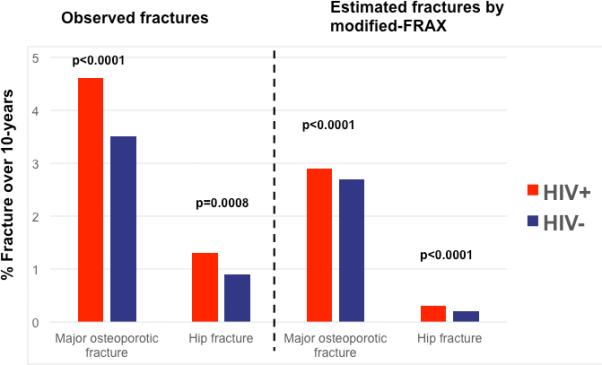
Background: FRAX is a validated, computer-based clinical fracture risk calculator that estimates the 10-year risk of major osteoporotic (clinical spine, forearm, hip, or shoulder) fracture, and hip fracture alone. It is widely used for decision making in fracture prevention, but it may underestimate the risk in HIV-infected individuals. Some experts recommend considering HIV as a cause of secondary osteoporosis when calculating FRAX in HIV-infected individuals.
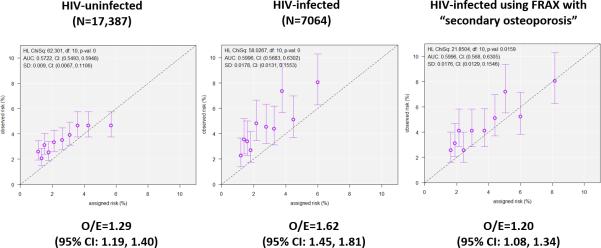
Methods: From the Veterans Aging Cohort Study Virtual Cohort, we included 24,451 HIV-infected and uninfected men aged 50-70 years with complete data in the year 2000 to approximate all but 2 factors (ie, history of secondary osteoporosis and parental hip fracture) for modified-FRAX calculation without bone density and 10-year observational data for incident fragility fracture. The accuracy of the modified-FRAX calculation was compared by the observed/estimated (O/E) ratios of fracture by HIV status.
Results: The accuracy of modified-FRAX was less for HIV-infected [O/E = 1.62, 95% confidence interval (CI) 1.45 to 1.81] than uninfected men (O/E = 1.29, 95% CI: 1.19 to 1.40), but improved when HIV was included as a cause of secondary osteoporosis (O/E = 1.20, 95% CI: 1.08 to 1.34). However, only 3%-6% of men with incident fractures were correctly identified by the modified-FRAX using accepted FRAX thresholds for pharmacologic therapy.
Conclusions: Modified-FRAX underestimated the fracture rates more in older HIV-infected than in otherwise similar uninfected men. The accuracy improved when HIV was included as a cause of secondary osteoporosis, but it still performed poorly for case finding. Further studies are necessary to determine how to use FRAX or define an HIV-specific index to risk stratify for screening and treatment in older HIV-infected individuals.
Figures
Similar articles
-
Improved fracture prediction using different fracture risk assessment tool adjustments in HIV-infected women.AIDS. 2018 Jul 31;32(12):1699-1706. doi: 10.1097/QAD.0000000000001864. AIDS. 2018. PMID: 29762165 Free PMC article.
-
Fracture Risk with Modified FRAX in Men Living with HIV.J Clin Densitom. 2024 Jan-Mar;27(1):101460. doi: 10.1016/j.jocd.2023.101460. Epub 2023 Dec 7. J Clin Densitom. 2024. PMID: 38128450
-
[Osteoporosis - whom to treat? The importance of FRAX® in Switzerland].Ther Umsch. 2012 Mar;69(3):207-13. doi: 10.1024/0040-5930/a000275. Ther Umsch. 2012. PMID: 22403115 German.
-
Primary care use of FRAX: absolute fracture risk assessment in postmenopausal women and older men.Postgrad Med. 2010 Jan;122(1):82-90. doi: 10.3810/pgm.2010.01.2102. Postgrad Med. 2010. PMID: 20107292 Review.
-
[Usefulness of FRAX and future issues in women's health].Clin Calcium. 2009 Dec;19(12):1742-8. Clin Calcium. 2009. PMID: 19949265 Review. Japanese.
Cited by
-
Bone health in HIV and hepatitis B or C infections.Ther Adv Musculoskelet Dis. 2017 Jan;9(1):22-34. doi: 10.1177/1759720X16671927. Epub 2016 Oct 7. Ther Adv Musculoskelet Dis. 2017. PMID: 28101146 Free PMC article. Review.
-
Osteoporosis in postmenopausal women living with HIV.Maturitas. 2017 Jan;95:50-54. doi: 10.1016/j.maturitas.2016.10.015. Epub 2016 Nov 5. Maturitas. 2017. PMID: 27889053 Free PMC article. Review.
-
Bone Loss in HIV Infection.Curr Treat Options Infect Dis. 2017 Mar;9(1):52-67. doi: 10.1007/s40506-017-0109-9. Epub 2017 Feb 23. Curr Treat Options Infect Dis. 2017. PMID: 28413362 Free PMC article.
-
Cost-effective osteoporosis treatment thresholds for people living with HIV infection in Greece.J Musculoskelet Neuronal Interact. 2017 Dec 1;17(4):292-298. J Musculoskelet Neuronal Interact. 2017. PMID: 29199188 Free PMC article.
-
Bone Loss and Fractures in Post-Menopausal Women Living with HIV: A Narrative Review.Pathogens. 2024 Sep 19;13(9):811. doi: 10.3390/pathogens13090811. Pathogens. 2024. PMID: 39339002 Free PMC article. Review.
References
-
- Young B, Dao CN, Buchacz K, Baker R, Brooks JT. Increased rates of bone fracture among HIV-infected persons in the HIV Outpatient Study (HOPS) compared with the US general population, 2000-2006. Clin Infect Dis. 2011 Apr 15;52(8):1061–1068. - PubMed
-
- Hansen AB, Gerstoft J, Kronborg G, et al. Incidence of low- and high-energy fractures in persons with and without HIV-infection: a Danish population-based cohort study. Aids. Nov 16. 2011 - PubMed
-
- Aberg JA, Gallant JE, Ghanem KG, et al. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2014 Jan;58(1):1–10. - PubMed
-
- European AIDS Clinical Society Treatment Guidelines. 2015; Version 8.0. 2015 http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html.
Publication types
MeSH terms
Grants and funding
- U24 AA022001/AA/NIAAA NIH HHS/United States
- K01 NR013437/NR/NINR NIH HHS/United States
- P30 MH062294/MH/NIMH NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U24 AA022007/AA/NIAAA NIH HHS/United States
- R01 HL090342/HL/NHLBI NIH HHS/United States
- R01 AI095089/AI/NIAID NIH HHS/United States
- R01 HS018372/HS/AHRQ HHS/United States
- U01 AA020795/AA/NIAAA NIH HHS/United States
- R01 CA173754/CA/NCI NIH HHS/United States
- U10 AA013566/AA/NIAAA NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- R01 HD073977/HD/NICHD NIH HHS/United States
- U01 AA020799/AA/NIAAA NIH HHS/United States
- R01 HL095136/HL/NHLBI NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- R01 DA035616/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
