

Mineral and bone disorders, morbidity and mortality in end-stage renal failure patients on chronic dialysis
- PMID: 27004031
- PMCID: PMC4777475
- DOI: 10.15386/cjmed-515
Mineral and bone disorders, morbidity and mortality in end-stage renal failure patients on chronic dialysis
Abstract
Background and aim: In spite of numerous interventions, the control of mineral disturbances remains poor in end-stage renal failure (ESRF) patients. Chronic kidney disease - mineral and bone disorders (CKD-MBD) represent an important cause of mortality and morbidity. The aim of this study is to analyze the relationship between mineral and bone disorders (MBD) and their components impact on all-cause mortality and cardiovascular (CDV) mortality and morbidity in chronic dialysis patients.
Methods: This prospective study was carried out in a cohort of 92 randomly selected patients with ESRF treated with hemodialysis (HD) and peritoneal dialysis (PD). The data regarding demographic and clinical characteristics were recorded, including vascular disease (coronary, cerebral, peripheral). The follow-up lasted 40 months and the final evaluation included the number and causes of deaths, CDV events and disease. Serum Ca, P, ALP, iPTH, albumin, cholesterol, urea and creatinine levels were measured. The plain radiographic films of hands and pelvis evaluated all bone abnormalities suggestive of renal osteodystrophy (ROD) and peripheral vascular calcification (VC).
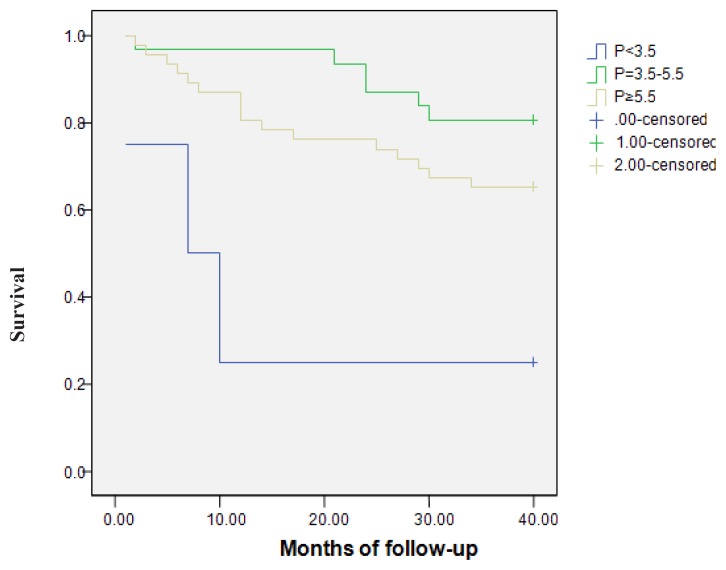
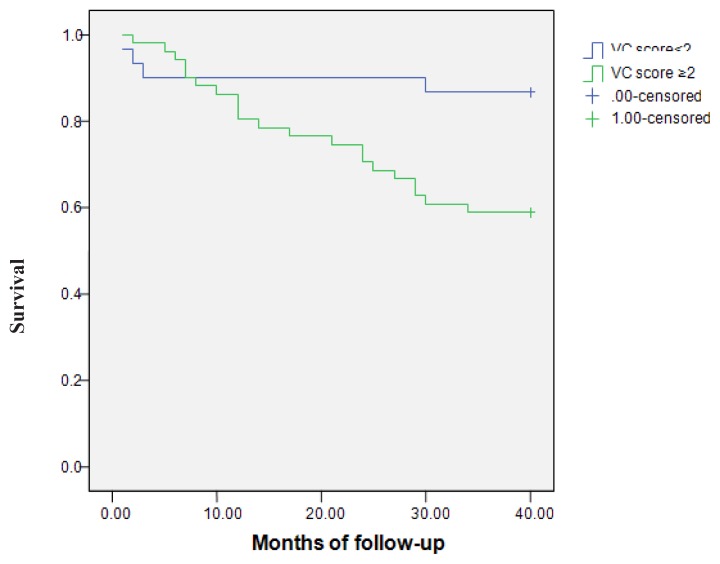
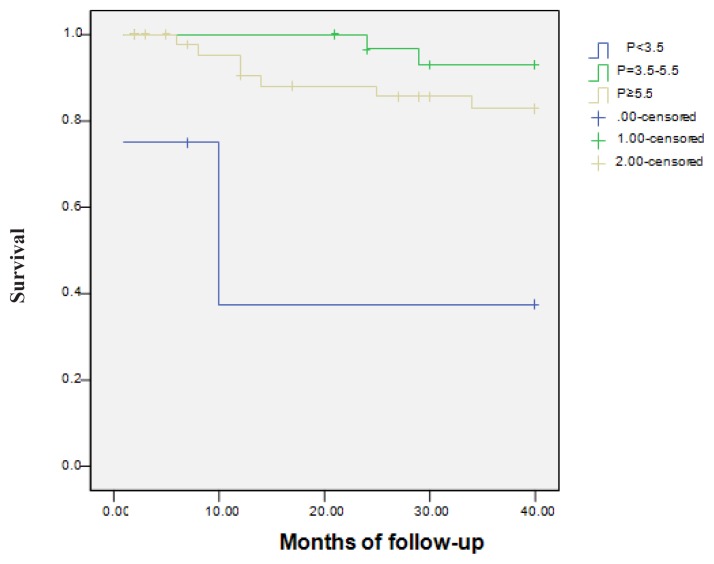
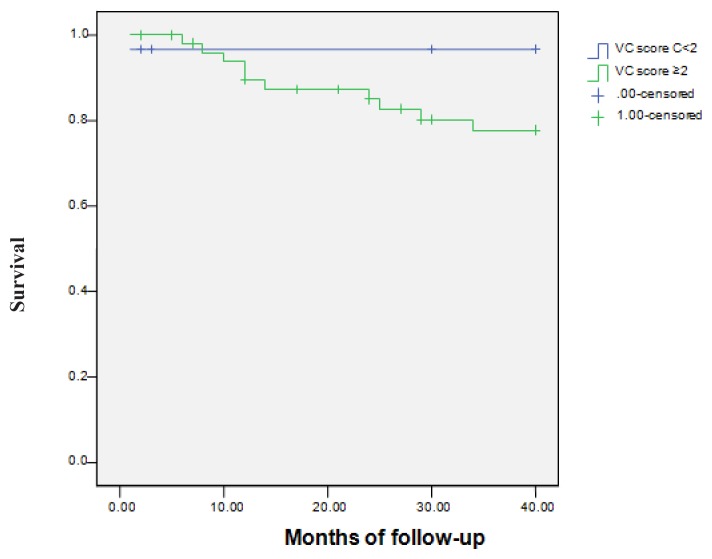
Results: All-cause annual mortality represented 9.25% in HD and 9.09% in PD patients. The CDV mortality represented almost 44% in HD patients and 66% in PD patients from all deaths. There was a high prevalence of CDV diseases and events. High and low serum P levels were associated with a worse survival rate. Hypercalcaemia was associated with high risk for CDV events in HD patients. In PD patients, the relationship between increased ALP levels and all-cause mortality was significant. Other mineral markers were not predictive of the outcome in the studied patients. In the HD patients the severity of VC was associated with all-cause and CDV mortality, and with CDV events. Male gender, hypercholesterolemia, decreased URR, albumin and creatinine were identified as risk factors for all-cause mortality. The diabetics had higher death rates. Low dialysis efficacy represented a risk factor for mortality and CDV diseases and events. In PD patients, low albumin induced a higher death rate. In PD patients the death rate was similar to HD patients.
Conclusion: All-cause mortality was higher than in general population, but lower than the chronic dialysis patients' mortality reported in other studies. The death rates in HD and PD patients were similar. VC and serum P levels influenced the outcome in the HD patients - increased the risk for all-cause and CDV mortality, but also for CDV events. ALP levels influenced outcome in PD patients. There were no significant differences between HD and PD patients regarding outcome.
Keywords: cardiovascular events; chronic dialysis; mineral and bone disorders; morbidity; mortality; renalosteodystrophy; vascular calcification.
Figures
References
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15:2208–2218. - PubMed
-
- Stevens LA, Djurdjev O, Cardew S, Cameron EC, Levin A. Calcium, phosphate, and parathyroid hormone levels in combination and as a function of dialysis duration predict mortality: evidence for the complexity of the association between mineral metabolism and outcomes. J Am Soc Nephrol. 2004;15:770–779. - PubMed
-
- Jean G, Bresson E, Terrat JC, Vanel T, Hurot JM, Lorriaux C, et al. Peripheral vascular calcification in long-haemodialysis patients: associated factors and survival consequences. Nephrol Dial Transplant. 2009;4(3):948–955. - PubMed
-
- Adragao T, Pires A, Lucas C, Birne R, Magalhaes L, Gonçalves M, et al. A simple vascular calcification score predicts cardiovascular risk in haemodialysis patients. Nephrol Dial Transplant. 2004;19:1480–1488. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources