

Antidepressant use and risk of cardiovascular outcomes in people aged 20 to 64: cohort study using primary care database
- PMID: 27005565
- PMCID: PMC4804126
- DOI: 10.1136/bmj.i1350
Antidepressant use and risk of cardiovascular outcomes in people aged 20 to 64: cohort study using primary care database
Abstract
Objective: To assess associations between different antidepressant treatments and rates of three cardiovascular outcomes (myocardial infarction, stroke or transient ischaemic attack, and arrhythmia) in people with depression.
Design: Cohort study.
Setting: UK general practices contributing to the QResearch primary care database.
Participants: 238,963 patients aged 20 to 64 years with a first diagnosis of depression between 1 January 2000 and 31 July 2011.
Exposures: Antidepressant class (tricyclic and related antidepressants, selective serotonin reuptake inhibitors, other antidepressants), dose, duration of use, and commonly prescribed individual antidepressant drugs.
Main outcome measures: First diagnoses of myocardial infarction, stroke or transient ischaemic attack, and arrhythmia during five years' follow-up. Cox proportional hazards models were used to estimate hazard ratios, adjusting for potential confounding variables.
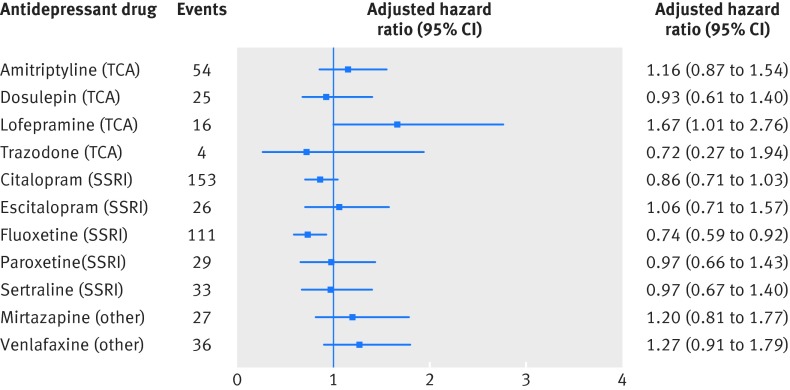
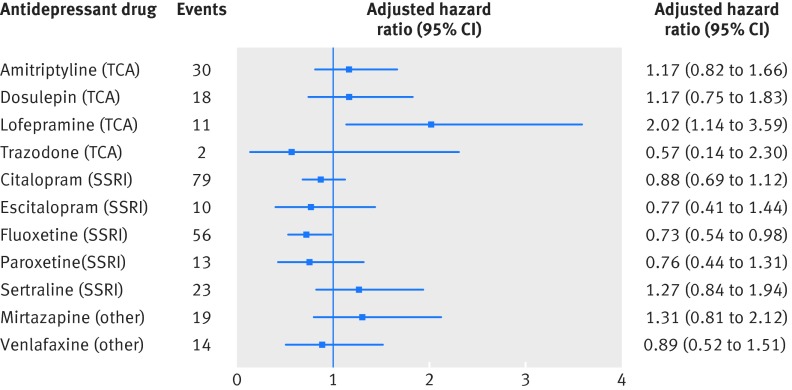
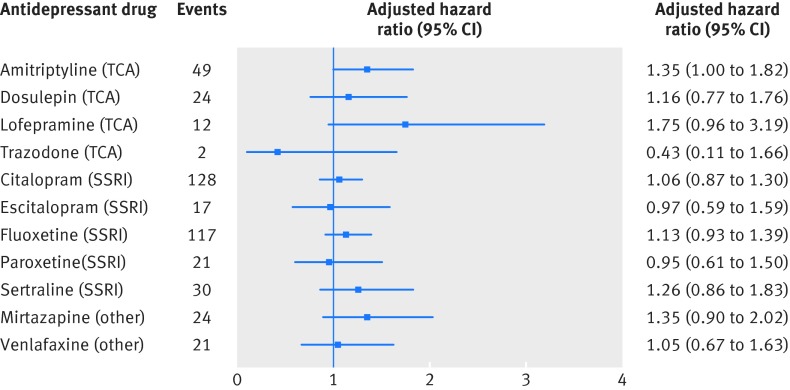
Results: During five years of follow-up, 772 patients had a myocardial infarction, 1106 had a stroke or transient ischaemic attack, and 1452 were diagnosed as having arrhythmia. No significant associations were found between antidepressant class and myocardial infarction over five years' follow-up. In the first year of follow-up, patients treated with selective serotonin reuptake inhibitors had a significantly reduced risk of myocardial infarction (adjusted hazard ratio 0.58, 95% confidence interval 0.42 to 0.79) compared with no use of antidepressants; among individual drugs, fluoxetine was associated with a significantly reduced risk (0.44, 0.27 to 0.72) and lofepramine with a significantly increased risk (3.07, 1.50 to 6.26). No significant associations were found between antidepressant class or individual drugs and risk of stroke or transient ischaemic attack. Antidepressant class was not significantly associated with arrhythmia over five years' follow-up, although the risk was significantly increased during the first 28 days of treatment with tricyclic and related antidepressants (adjusted hazard ratio 1.99, 1.27 to 3.13). Fluoxetine was associated with a significantly reduced risk of arrhythmia (0.74, 0.59 to 0.92) over five years, but citalopram was not significantly associated with risk of arrhythmia even at high doses (1.11, 0.72 to 1.71 for doses ≥ 40 mg/day).
Conclusions: This study found no evidence that selective serotonin reuptake inhibitors are associated with an increased risk of arrhythmia or stroke/transient ischaemic attack in people diagnosed as having depression between the ages of 20 to 64 or that citalopram is associated with a significantly increased risk of arrhythmia. It found some indication of a reduced risk of myocardial infarction with selective serotonin reuptake inhibitors, particularly fluoxetine, and of an increased risk with lofepramine.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
In adults < 65 years of age, antidepressant drugs were not linked to increased risk for CV outcomes.Ann Intern Med. 2016 Jul 19;165(2):JC10. doi: 10.7326/ACPJC-2016-165-2-010. Ann Intern Med. 2016. PMID: 27429312 No abstract available.
References
-
- Hatcher S, Arroll B. Newer antidepressants for the treatment of depression in adults. BMJ 2012;344:d8300. - PubMed
-
- Jolly K, Langman MJS. Psychotropic medication: curing illness or creating problems?Heart 2009;95:1893-4. - PubMed
-
- Olfson M, Marcus SC. National patterns in antidepressant medication treatment. Arch Gen Psychiatry 2009;66:848-56. - PubMed
-
- Stephenson CP, Karanges E, McGregor IS. Trends in the utilisation of psychotropic medications in Australia from 2000 to 2011. Aust N Z J Psychiatry 2013;47:74-87. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical