

Plasma Levels of Risk-Variant APOL1 Do Not Associate with Renal Disease in a Population-Based Cohort
- PMID: 27005919
- PMCID: PMC5042671
- DOI: 10.1681/ASN.2015101121
Plasma Levels of Risk-Variant APOL1 Do Not Associate with Renal Disease in a Population-Based Cohort
Abstract
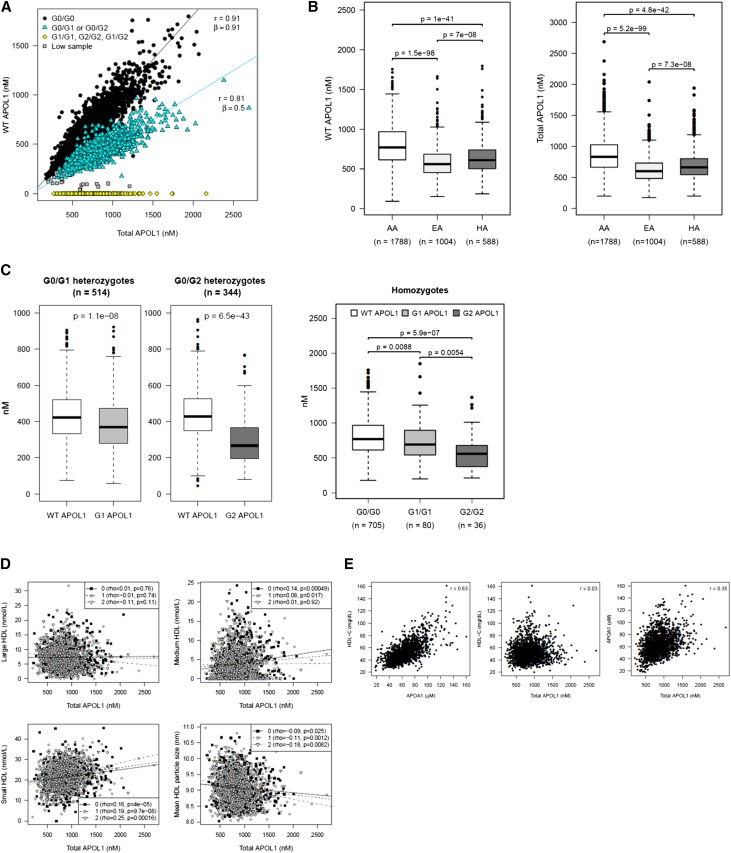
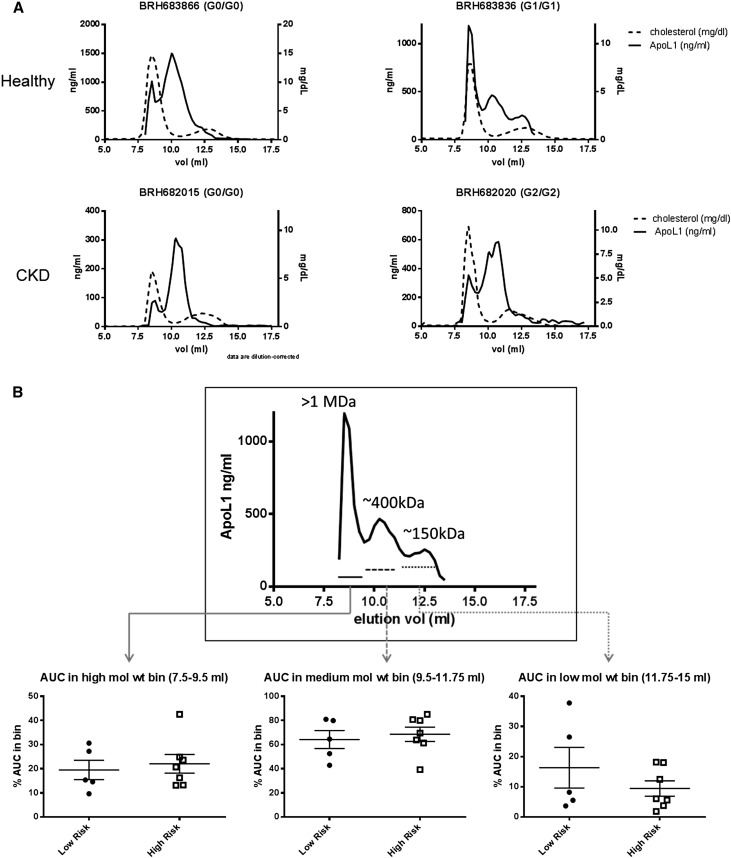
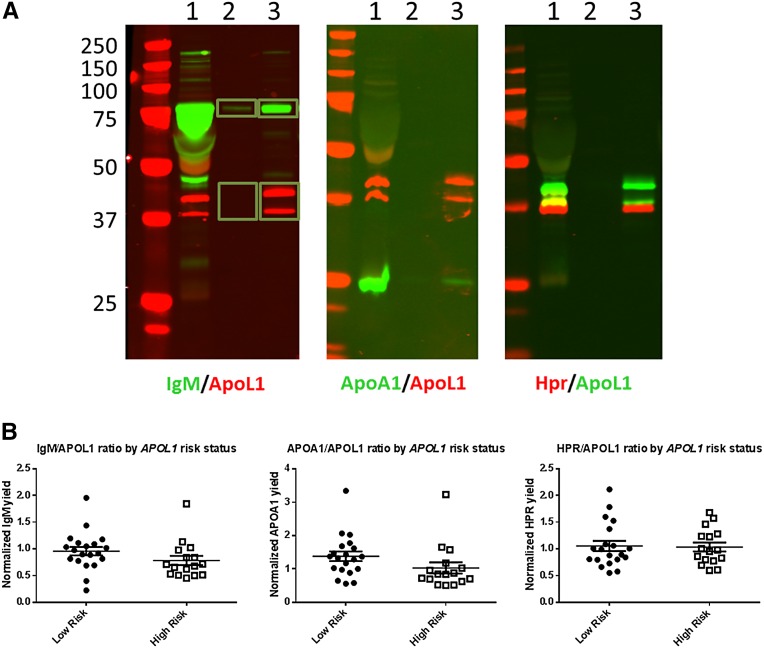
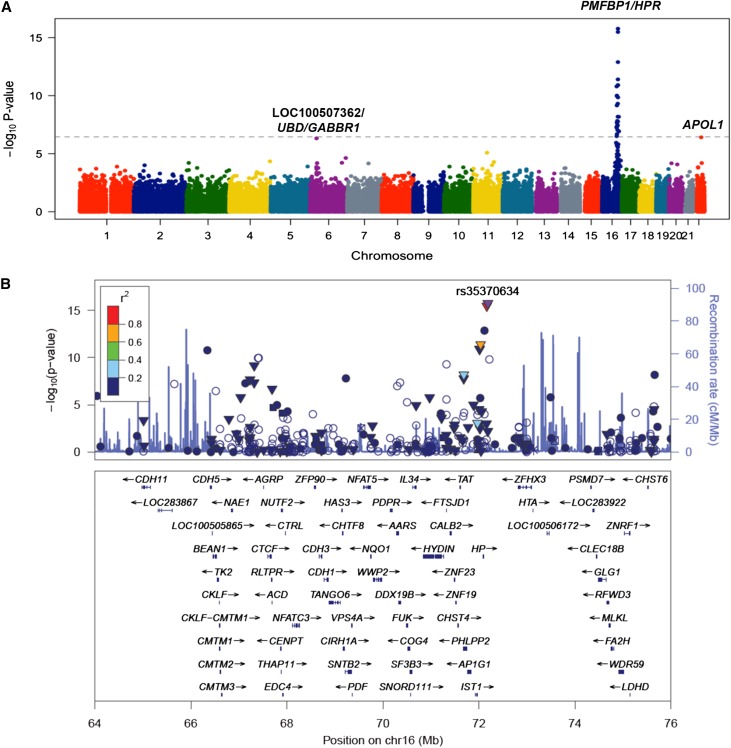
Two common missense variants in APOL1 (G1 and G2) have been definitively linked to CKD in black Americans. However, not all individuals with the renal-risk genotype develop CKD, and little is known about how APOL1 variants drive disease. Given the association of APOL1 with HDL particles, which are cleared by the kidney, differences in the level or quality of mutant APOL1‑HDL particles could be causal for disease and might serve as a useful risk stratification marker. We measured plasma levels of G0 (low risk), G1, and G2 APOL1 in 3450 individuals in the Dallas Heart Study using a liquid chromatography-MS method that enabled quantitation of the different variants. Additionally, we characterized native APOL1‑HDL from donors with no or two APOL1 risk alleles by size-exclusion chromatography and analysis of immunopurified APOL1‑HDL particles. Finally, we identified genetic loci associated with plasma APOL1 levels and tested for APOL1-dependent association with renal function. Although we replicated the previous association between APOL1 variant status and renal function in nondiabetic individuals, levels of circulating APOL1 did not associate with microalbuminuria or GFR. Furthermore, the size or known components of APOL1‑HDL did not consistently differ in subjects with the renal-risk genotype. Genetic association studies implicated variants in loci harboring haptoglobin-related protein (HPR), APOL1, and ubiquitin D (UBD) in the regulation of plasma APOL1 levels, but these variants did not associate with renal function. Collectively, these data demonstrate that the risk of renal disease associated with APOL1 is probably not related to circulating levels of the mutant protein.
Keywords: Epidemiology and outcomes; Pathophysiology of Renal Disease and Progression; chronic kidney disease; genetic renal disease; human genetics; risk factors.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Genovese G, Friedman DJ, Ross MD, Lecordier L, Uzureau P, Freedman BI, Bowden DW, Langefeld CD, Oleksyk TK, Uscinski Knob AL, Bernhardy AJ, Hicks PJ, Nelson GW, Vanhollebeke B, Winkler CA, Kopp JB, Pays E, Pollak MR: Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science 329: 841–845, 2010 - PMC - PubMed
-
- Freedman BI, Langefeld CD, Andringa KK, Croker JA, Williams AH, Garner NE, Birmingham DJ, Hebert LA, Hicks PJ, Segal MS, Edberg JC, Brown EE, Alarcón GS, Costenbader KH, Comeau ME, Criswell LA, Harley JB, James JA, Kamen DL, Lim SS, Merrill JT, Sivils KL, Niewold TB, Patel NM, Petri M, Ramsey-Goldman R, Reveille JD, Salmon JE, Tsao BP, Gibson KL, Byers JR, Vinnikova AK, Lea JP, Julian BA, Kimberly RP Lupus Nephritis–End‐Stage Renal Disease Consortium : End-stage renal disease in African Americans with lupus nephritis is associated with APOL1. Arthritis Rheumatol 66: 390–396, 2014 - PMC - PubMed
-
- Kopp JB, Nelson GW, Sampath K, Johnson RC, Genovese G, An P, Friedman D, Briggs W, Dart R, Korbet S, Mokrzycki MH, Kimmel PL, Limou S, Ahuja TS, Berns JS, Fryc J, Simon EE, Smith MC, Trachtman H, Michel DM, Schelling JR, Vlahov D, Pollak M, Winkler CA: APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J Am Soc Nephrol 22: 2129–2137, 2011 - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
