

Risk stratification of chromosomal abnormalities in chronic myelogenous leukemia in the era of tyrosine kinase inhibitor therapy
- PMID: 27006386
- PMCID: PMC4915795
- DOI: 10.1182/blood-2016-01-690230
Risk stratification of chromosomal abnormalities in chronic myelogenous leukemia in the era of tyrosine kinase inhibitor therapy
Abstract
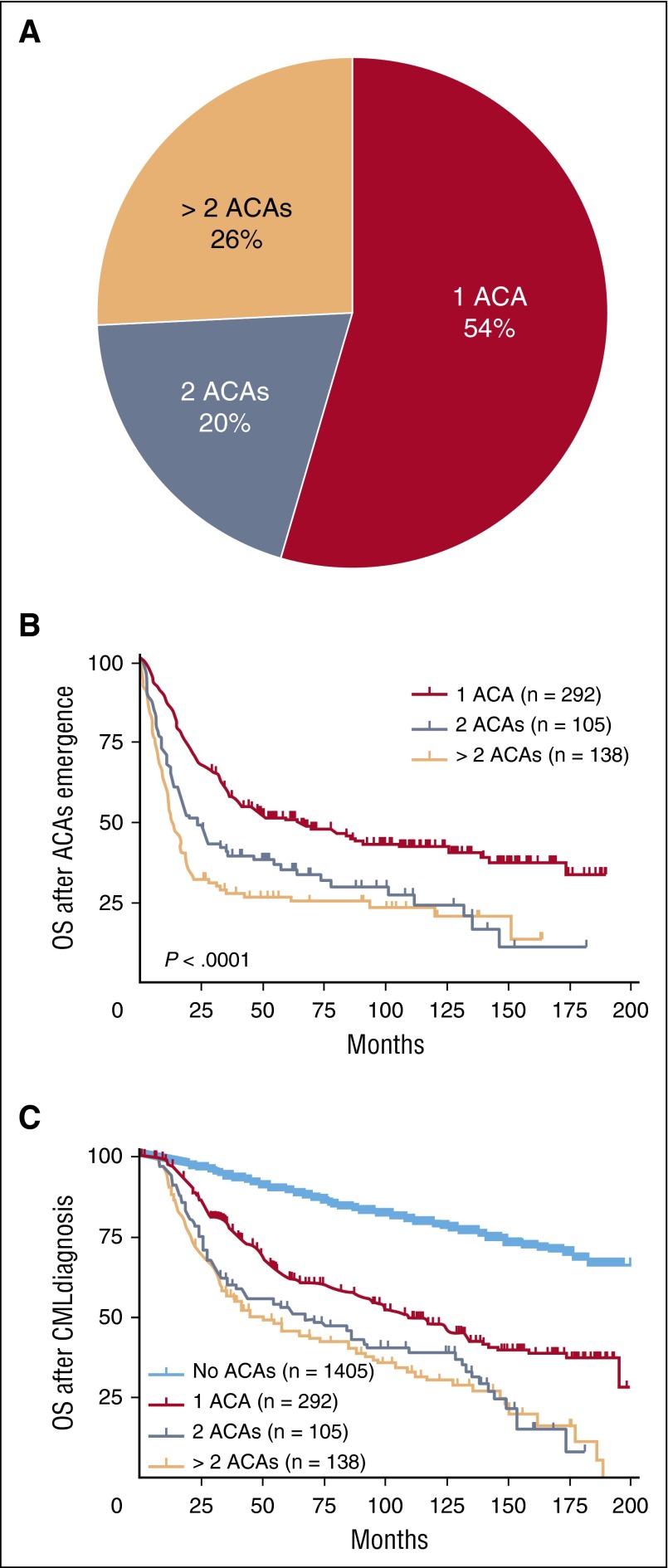
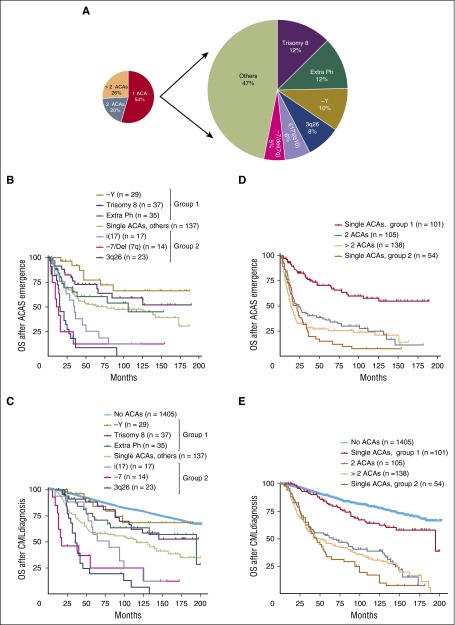
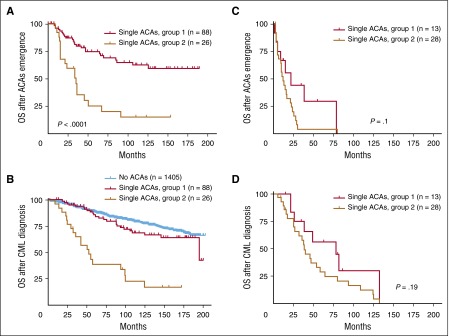
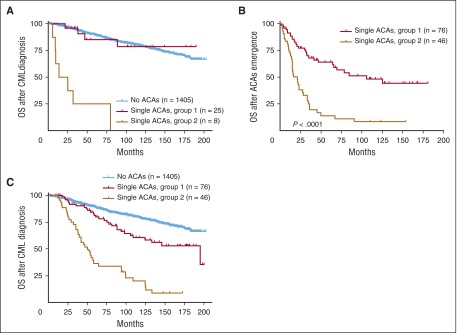
Clonal cytogenetic evolution with additional chromosomal abnormalities (ACAs) in chronic myelogenous leukemia (CML) is generally associated with decreased response to tyrosine kinase inhibitor (TKI) therapy and adverse survival. Although ACAs are considered as a sign of disease progression and have been used as one of the criteria for accelerated phase, the differential prognostic impact of individual ACAs in CML is unknown, and a classification system to reflect such prognostic impact is lacking. In this study, we aimed to address these questions using a large cohort of CML patients treated in the era of TKIs. We focused on cases with single chromosomal changes at the time of ACA emergence and stratified the 6 most common ACAs into 2 groups: group 1 with a relatively good prognosis including trisomy 8, -Y, and an extra copy of Philadelphia chromosome; and group 2 with a relatively poor prognosis including i(17)(q10), -7/del7q, and 3q26.2 rearrangements. Patients in group 1 showed much better treatment response and survival than patients in group 2. When compared with cases with no ACAs, ACAs in group 2 conferred a worse survival irrelevant to the emergence phase and time. In contrast, ACAs in group 1 had no adverse impact on survival when they emerged from chronic phase or at the time of CML diagnosis. The concurrent presence of 2 or more ACAs conferred an inferior survival and can be categorized into the poor prognostic group.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Cytogenetics in CML: more important than you think.Blood. 2016 Jun 2;127(22):2661-2. doi: 10.1182/blood-2016-04-708206. Blood. 2016. PMID: 27257178 No abstract available.
References
-
- Marktel S, Marin D, Foot N, et al. Chronic myeloid leukemia in chronic phase responding to imatinib: the occurrence of additional cytogenetic abnormalities predicts disease progression. Haematologica. 2003;88(3):260–267. - PubMed
-
- Grimwade D, Hills RK, Moorman AV, et al. National Cancer Research Institute Adult Leukaemia Working Group. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116(3):354–365. - PubMed
-
- Fioretos T, Johansson B. Chronic myeloid leukemia. In: Heim S, Mitelman F, editors. Cancer Cytogenetics. Hoboken, NJ: Wiley-Blackwell; 2009. pp. 179–207.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
