

The value of using a brain laser interstitial thermal therapy (LITT) system in patients presenting with high grade gliomas where maximal safe resection may not be feasible
- PMID: 27006643
- PMCID: PMC4802786
- DOI: 10.1186/s12962-016-0055-2
The value of using a brain laser interstitial thermal therapy (LITT) system in patients presenting with high grade gliomas where maximal safe resection may not be feasible
Abstract
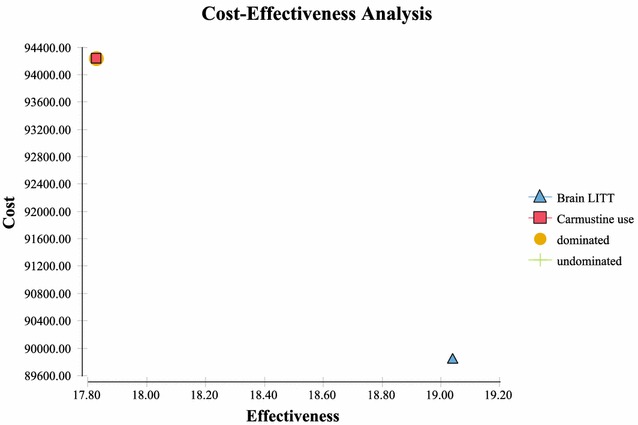
Background: The objective of this analysis was to determine the value (incremental cost/increment benefit) of a brain LITT system versus employing current surgical options recommended by NCCN guidelines, specifically open resection (i.e. craniotomy) methods or biopsy (collectively termed CURRENT TREATMENTS) in patients where maximal safe resection may not be feasible. As has been demonstrated in the literature, extent of resection/ablation with minimal complications are independently related to overall survival.
Methods: A cost effectiveness analysis from a societal perspective was employed using TreeAge Pro 2014 software. Direct costs (using national average Medicare reimbursement amounts), outcomes (overall survival), and value [defined as increment cost/incremental survival-evaluated as cost/life year gained (LYG)] were evaluated. Sensitivity analysis was also performed to determine which variables had the largest effect on incremental costs and outcomes.
Results: In the base case, the overall survival was improved with brain LITT versus CURRENT TREATMENTS by 3.07 months at an additional cost of $7508 (or $29,340/LYG). This amount was significantly less than the current international threshold value for $32,575/LYG and considerably less than the US threshold value of $50,000/LYG. This incremental cost may also qualify under NICE criteria for end of life therapies. In sensitivity analysis: As percent local recurrence GBM increased; cost of DRG25/26 increased; percent GTR increased; and gliadel use increased-the value of brain LITT improved. Additionally, in those patients where a biopsy is the only option, brain LITT extended life by 7 months.
Conclusions: Brain LITT should be considered a viable option for treatment of high grade gliomas as it improves survival at a cost which appears to be of good value to society. This incremental cost is less than the international and US thresholds for good value.
Keywords: Brain LITT; Cost effectiveness; LYG; Survival; Value.
Figures







References
-
- Central Brain Tumor Registry of the United States (CBTRUS). 2014. http://www.cbtrus.org/reports/reports.html. Accessed 29 Apr 2015.
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OM, Zanella F, Ruelen H-J, ALA-Glioma Study Group Flourescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomized controlled multicentre phase III trial. Lancet Oncol. 2006;7:392–401. doi: 10.1016/S1470-2045(06)70665-9. - DOI - PubMed
-
- Ostrom QT, Gittleman H, Liao P, Rouse C, Chen Y, Dowling J, Wolinsky Y, Krucho C, Barnholtz-Sloan J. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro-Oncol. 2014;16:iv1–iv63. doi: 10.1093/neuonc/nou223. - DOI - PMC - PubMed
-
- Almenawer SA, Badhiwala JH, Alhazzani W, Greenspoon J, Farrokhyar F, Yarascavitch B, Algird A, Kachur E, Cenic A, Sharieff W, Klurfan P, Gunnarsson T, Ajani O, Reddy K, Singh SK, Murty NK. Biopsy versus partial versus gross total resection in older patients with high-grade glioma: a systematic review and meta-analysis. Neuro-Oncol. 2015 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
