

Perioperative sleep apnea: a real problem or did we invent a new disease?
- PMID: 27006758
- PMCID: PMC4797892
- DOI: 10.12688/f1000research.7218.1
Perioperative sleep apnea: a real problem or did we invent a new disease?
Abstract
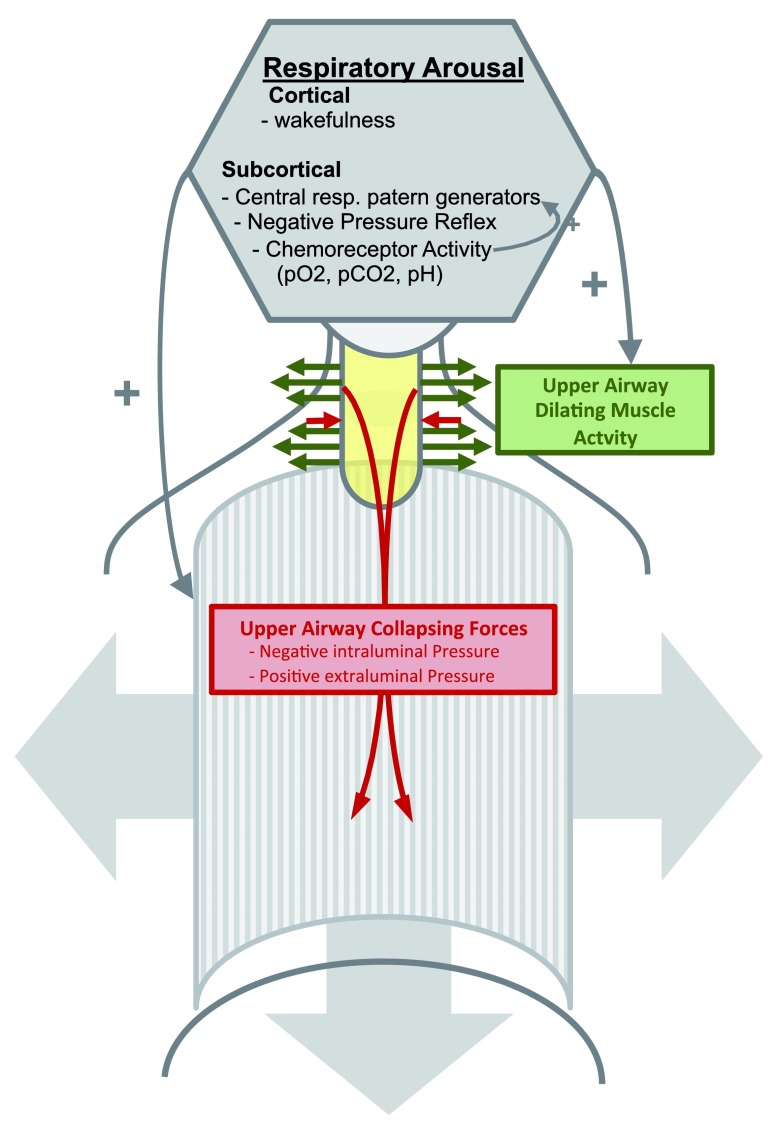
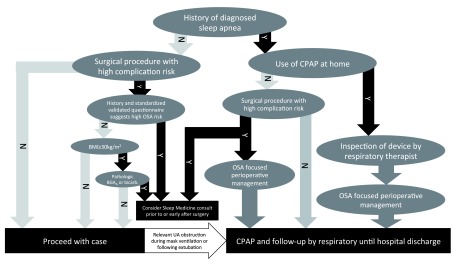
Depending on the subpopulation, obstructive sleep apnea (OSA) can affect more than 75% of surgical patients. An increasing body of evidence supports the association between OSA and perioperative complications, but some data indicate important perioperative outcomes do not differ between patients with and without OSA. In this review we will provide an overview of the pathophysiology of sleep apnea and the risk factors for perioperative complications related to sleep apnea. We also discuss a clinical algorithm for the identification and management of OSA patients facing surgery.
Keywords: Anaesthesiology; Bariatric surgery; Obstructive sleep apnea; Perioperative sleep apnea; Upper airway.
Conflict of interest statement
James E. Mojica declares that he has no disclosures.
No competing interests were disclosed.
Figures
Similar articles
-
Obstructive Sleep Apnea and the Adult Perioperative Patient.J Perianesth Nurs. 2015 Dec;30(6):528-545. doi: 10.1016/j.jopan.2014.07.014. Epub 2015 Sep 1. J Perianesth Nurs. 2015. PMID: 26596388
-
Obstructive sleep apnea in the perioperative setting: complications and management strategies.Hosp Pract (1995). 2015;43(1):56-63. doi: 10.1080/21548331.2015.1001709. Epub 2015 Jan 6. Hosp Pract (1995). 2015. PMID: 25559851 Review.
-
Obstructive Sleep Apnea-a Perioperative Risk Factor.Dtsch Arztebl Int. 2016 Jul 11;113(27-28):463-9. doi: 10.3238/arztebl.2016.0463. Dtsch Arztebl Int. 2016. PMID: 27476705 Free PMC article. Review.
-
Is obstructive sleep apnea associated with difficult airway? Evidence from a systematic review and meta-analysis of prospective and retrospective cohort studies.PLoS One. 2018 Oct 4;13(10):e0204904. doi: 10.1371/journal.pone.0204904. eCollection 2018. PLoS One. 2018. PMID: 30286122 Free PMC article.
-
Preoperatively Screened Obstructive Sleep Apnea Is Associated With Worse Postoperative Outcomes Than Previously Diagnosed Obstructive Sleep Apnea.Anesth Analg. 2017 Aug;125(2):593-602. doi: 10.1213/ANE.0000000000002241. Anesth Analg. 2017. PMID: 28682951
Cited by
-
Moderate-to-high risk of obstructive sleep apnea with excessive daytime sleepiness is associated with postoperative neurocognitive disorders: a prospective one-year follow-up cohort study.Front Neurosci. 2023 May 31;17:1161279. doi: 10.3389/fnins.2023.1161279. eCollection 2023. Front Neurosci. 2023. PMID: 37325036 Free PMC article.
-
Aneurysm size and blood pressure severity in patients with intracranial aneurysms and sleep apnea.J Clin Sleep Med. 2022 Jun 1;18(6):1539-1545. doi: 10.5664/jcsm.9906. J Clin Sleep Med. 2022. PMID: 35088709 Free PMC article.
-
Protocol of a multicentre, prospective cohort study that evaluates cost-effectiveness of two perioperative care strategies for potential obstructive sleep apnoea in morbidly obese patients undergoing bariatric surgery.BMJ Open. 2020 Oct 7;10(10):e038830. doi: 10.1136/bmjopen-2020-038830. BMJ Open. 2020. PMID: 33033026 Free PMC article.
-
A Brief Review of Non-invasive Monitoring of Respiratory Condition for Extubated Patients with or at Risk for Obstructive Sleep Apnea after Surgery.Front Med (Lausanne). 2017 Mar 8;4:26. doi: 10.3389/fmed.2017.00026. eCollection 2017. Front Med (Lausanne). 2017. PMID: 28337439 Free PMC article. Review.
-
Recent advances in understanding and managing postoperative respiratory problems.F1000Res. 2019 Feb 18;8:F1000 Faculty Rev-197. doi: 10.12688/f1000research.16687.1. eCollection 2019. F1000Res. 2019. PMID: 30828433 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources