

A Canadian population-based description of the indications for lower-extremity amputations and outcomes
- PMID: 27007090
- PMCID: PMC4814278
- DOI: 10.1503/cjs.013115
A Canadian population-based description of the indications for lower-extremity amputations and outcomes
Abstract
Background: To our knowledge, there have been no previously published reports characterizing lower-extremity amputations in Canada. The objective of this study was to describe the indications and outcomes of lower-extremity amputations in the Canadian population.
Methods: We performed a retrospective cohort study of all adult patients who underwent lower-extremity amputation in Canada between 2006 and 2009. Patients were identified from the Canadian Institute for Health Information's Discharge Abstract Database, which includes all hospital admissions across Canada with the exception of the province of Quebec. Pediatric, trauma, and outpatients were excluded.
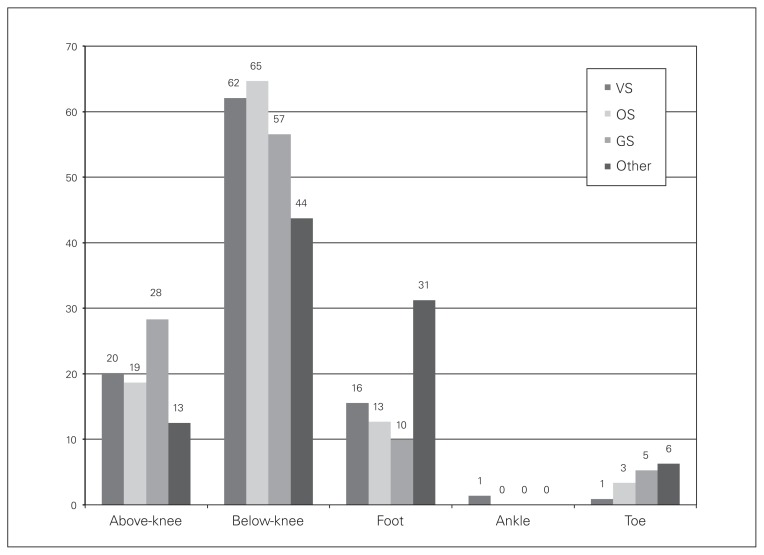
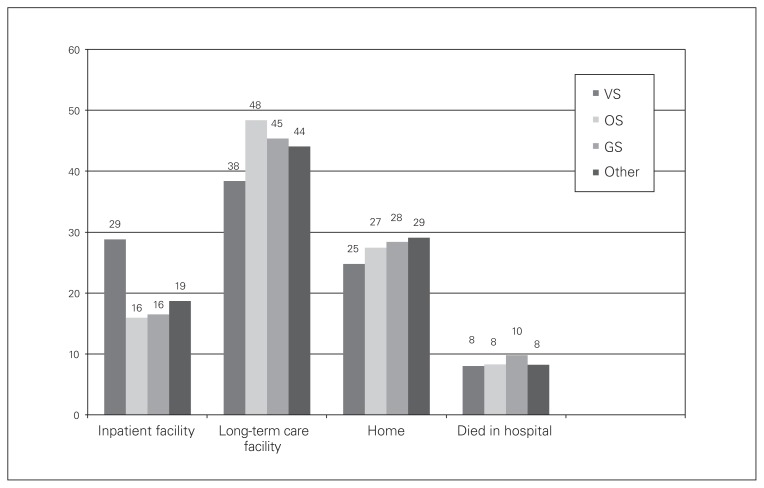
Results: During the study period, 5342 patients underwent lower-extremity amputations in 207 Canadian hospitals. The mean age was 67 ± 13 years, and 68% were men. Amputations were most frequently indicated after admission for diabetic complications (81%), cardiovascular disease (6%), or cancer (3%). In total, 65% of patients were discharged to another inpatient or long-term care facility, and 26% were discharged home with or without extra support. Most patients were diabetic (96%) and most (65%) required a below-knee amputation. Predictors of prolonged (> 7 d) hospital stay included amputation performed by a general surgeon; cardiovascular risk factors, such as diabetes, hypertension, ischemic heart disease, congestive heart failure, or hyperlipidemia; and undergoing the amputation in the provinces of Newfoundland and Labrador, New Brunswick, or British Columbia.
Conclusion: There is variability in the delivery of lower-extremity amputations and postoperative hospital discharges among surgical specialists and regions across Canada. Future work is needed to investigate the reasons for this variability and to develop initiatives to shorten postoperative hospital stays.
Contexte: À notre connaissance, aucun rapport caractérisant les amputations des membres inférieurs n’a été publié au Canada à ce jour. L’objectif de la présente étude était de décrire les indications et les résultats de ces amputations dans la population canadienne.
Méthodes: Nous avons effectué une étude de cohorte rétrospective portant sur tous les patients adultes ayant subi l’amputation d’un membre inférieur au Canada entre 2006 et 2009. Les patients ont été sélectionnés à partir de la Base de données sur les congés des patients de l’Institut canadien d’information sur la santé, qui comprend toutes les hospitalisations au Canada, à l’exception du Québec. Les cas pédiatriques, les traumatismes et les patients externes ont été exclus.
Résultants: Durant la période à l’étude, 5342 patients ont subi l’amputation d’un membre inférieur dans 207 hôpitaux canadiens. L’âge moyen était de 67 ± 13 ans, et 68 % des patients étaient des hommes. Les amputations étaient principalement recommandées après l’hospitalisation pour des complications du diabète (81 %), une maladie cardiovasculaire (6 %) ou un cancer (3 %). Au total, 65 % des patients ont été transférés vers un autre établissement hospitalier ou de soins de longue durée après leur congé, et 26 % sont retournés à la maison avec ou sans soutien supplémentaire. La plupart des patients étaient diabétiques (96 %), et la plupart (65 %) ont subi une amputation sous le genou. Les indicateurs d’hospitalisation longue (> 7 jours) comprenaient l’amputation par un chirurgien généraliste; les facteurs de risque cardiovasculaires, comme le diabète, l’hypertension, la cardiopathie ischémique, l’insuffisance cardiaque congestive ou l’hyperlipidémie; et le fait d’avoir subi l’amputation à Terre-Neuve-et-Labrador, au Nouveau-Brunswick ou en Colombie-Britannique.
Conclusion: La prestation de l’amputation d’un membre inférieur et le moment du congé postopératoire varient selon les chirurgiens et les régions du Canada. D’autres recherches seront nécessaires pour déterminer les raisons de cette variabilité et mettre en place des stratégies pour raccourcir les séjours hospitaliers postopératoires.
Figures
Comment in
-
Major lower-extremity amputations in diabetes: a response to "A Canadian population-based description of the indications for lower-extremity amputations and outcomes".Can J Surg. 2017 Oct;60(5):E4. doi: 10.1503/cjs.1760052. Can J Surg. 2017. PMID: 28930039 Free PMC article. No abstract available.
-
Major lower-extremity amputations in diabetes: a response to "A Canadian population-based description of the indications for lower-extremity amputations and outcomes": Author response.Can J Surg. 2017 Oct;60(5):E4. doi: 10.1503/cjs.1760053. Can J Surg. 2017. PMID: 28930040 Free PMC article. No abstract available.
References
-
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, et al. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89:422–9. - PubMed
-
- Ephraim PL, Dillingham TR, Sector M, et al. Epidemiology of limb loss and congenital limb deficiency: a review of the literature. Arch Phys Med Rehabil. 2003;84:747–61. - PubMed
-
- Moxey PW, Gogalniceanu P, Hinchliffe RJ, et al. Lower extremity amputations — a review of global variability in incidence. Diabet Med. 2011;28:1144–53. - PubMed
-
- Schofield CJ, Libby G, Brennan GM, et al. Mortality and hospitalization in patients after amputation: a comparison between patients with and without diabetes. Diabetes Care. 2006;29:2252–6. - PubMed