

The Role of Color and Morphologic Characteristics in Dermoscopic Diagnosis
- PMID: 27007917
- PMCID: PMC5473029
- DOI: 10.1001/jamadermatol.2016.0270
The Role of Color and Morphologic Characteristics in Dermoscopic Diagnosis
Abstract
Importance: Both colors and structures are considered important in the dermoscopic evaluation of skin lesions but their relative significance is unknown.
Objective: To determine if diagnostic accuracy for common skin lesions differs between gray-scale and color dermoscopic images.
Design, setting, and participants: A convenience sample of 40 skin lesions (8 nevi, 8 seborrheic keratoses, 7 basal cell carcinomas, 7 melanomas, 4 hemangiomas, 4 dermatofibromas, 2 squamous cell carcinomas [SCCs]) was selected and shown to attendees of a dermoscopy course (2014 Memorial Sloan Kettering Cancer Center dermoscopy course). Twenty lesions were shown only once, either in gray-scale (n = 10) or color (n = 10) (nonpaired). Twenty lesions were shown twice, once in gray-scale (n = 20) and once in color (n = 20) (paired). Participants provided their diagnosis and confidence level for each of the 60 images. Of the 261 attendees, 158 participated (60.5%) in the study. Most were attending physicians (n = 76 [48.1%]). Most participants were practicing or training in dermatology (n = 144 [91.1%]). The median (interquartile range) experience evaluating skin lesions and using dermoscopy of participants was 6 (13.5) and 2 (4.0) years, respectively.
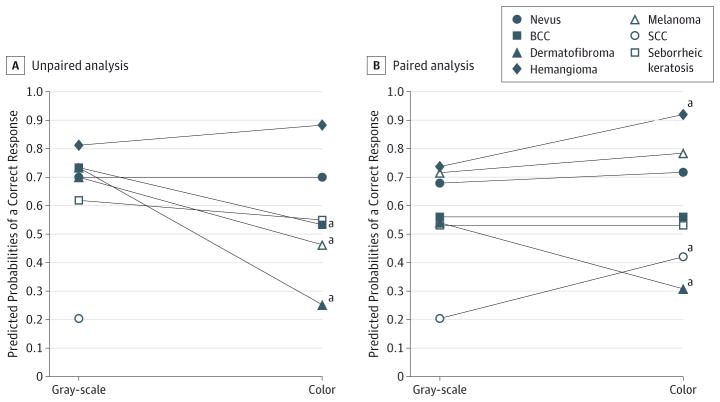
Main outcomes and measures: Diagnostic accuracy and confidence level of participants evaluating gray-scale and color images. Two separate analyses were performed: (1) an unpaired evaluation comparing gray-scale and color images shown either once or for the first time, and (2) a paired evaluation comparing pairs of gray-scale and color images of the same lesion.
Results: In univariate analysis of unpaired images, color images were less likely to be diagnosed correctly compared with gray-scale images (odds ratio [OR], 0.8; P < .001). Using gray-scale images as the reference, multivariate analyses of both unpaired and paired images found no association between correct lesion diagnosis and use of color images (OR, 1.0; P = .99, and OR, 1.2; P = .82, respectively). Stratified analysis of paired images using a color by diagnosis interaction term showed that participants were more likely to make a correct diagnosis of SCC and hemangioma in color (P < .001 for both comparisons) and dermatofibroma in gray-scale (P < .001).
Conclusions and relevance: Morphologic characteristics (ie, structures and patterns), not color, provide the primary diagnostic clue in dermoscopy. Use of gray-scale images may improve teaching of dermoscopy to novices by emphasizing the evaluation of morphology.
Conflict of interest statement
Figures
References
-
- Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002;3(3):159–165. - PubMed
-
- Bafounta ML, Beauchet A, Aegerter P, Saiag P. Is dermoscopy (epiluminescence microscopy) useful for the diagnosis of melanoma? results of a meta-analysis using techniques adapted to the evaluation of diagnostic tests. Arch Dermatol. 2001;137(10):1343–1350. - PubMed
-
- Vestergaard ME, Macaskill P, Holt PE, Menzies SW. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159(3):669–676. - PubMed
-
- Blum A, Hofmann-Wellenhof R, Luedtke H, et al. Value of the clinical history for different users of dermoscopy compared with results of digital image analysis. J Eur Acad Dermatol Venereol. 2004;18(6):665–669. - PubMed
-
- Marghoob AA, Scope A. The complexity of diagnosing melanoma. J Invest Dermatol. 2009;129(1):11–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
