

A Meta-Analysis of the Metabolic Syndrome Prevalence in the Global HIV-Infected Population
- PMID: 27008536
- PMCID: PMC4805252
- DOI: 10.1371/journal.pone.0150970
A Meta-Analysis of the Metabolic Syndrome Prevalence in the Global HIV-Infected Population
Abstract
Background: Cardio-metabolic risk factors are of increasing concern in HIV-infected individuals, particularly with the advent of antiretroviral therapy (ART) and the subsequent rise in longevity. However, the prevalence of cardio-metabolic abnormalities in this population and the differential contribution, if any, of HIV specific factors to their distribution, are poorly understood. Therefore, we conducted a systematic review and meta-analysis to estimate the global prevalence of metabolic syndrome (MS) in HIV-infected populations, its variation by the different diagnostic criteria, severity of HIV infection, ART used and other major predictive characteristics.
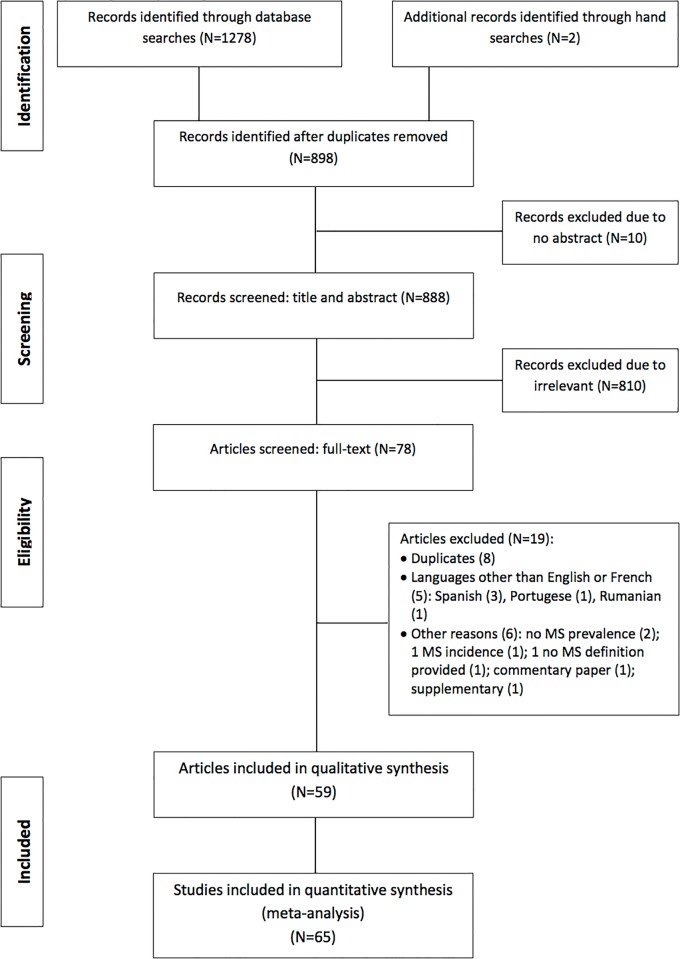
Methods: We performed a comprehensive search on major databases for original research articles published between 1998 and 2015. The pooled overall prevalence as well as by specific groups and subgroups were computed using random effects models.
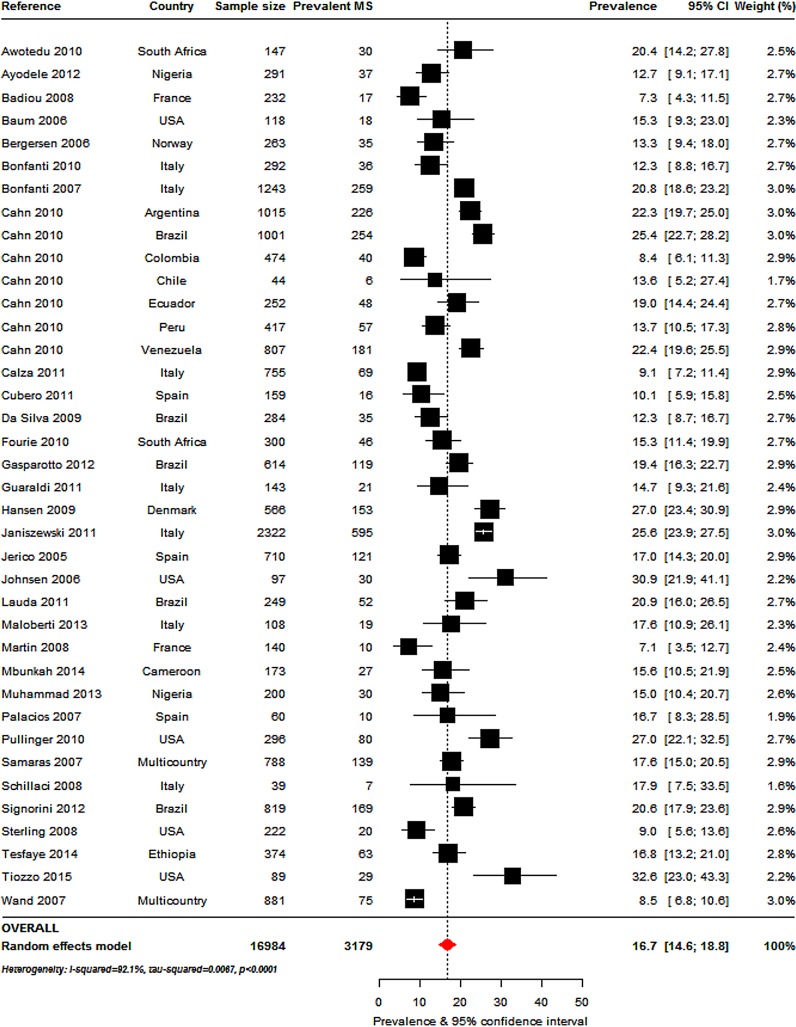
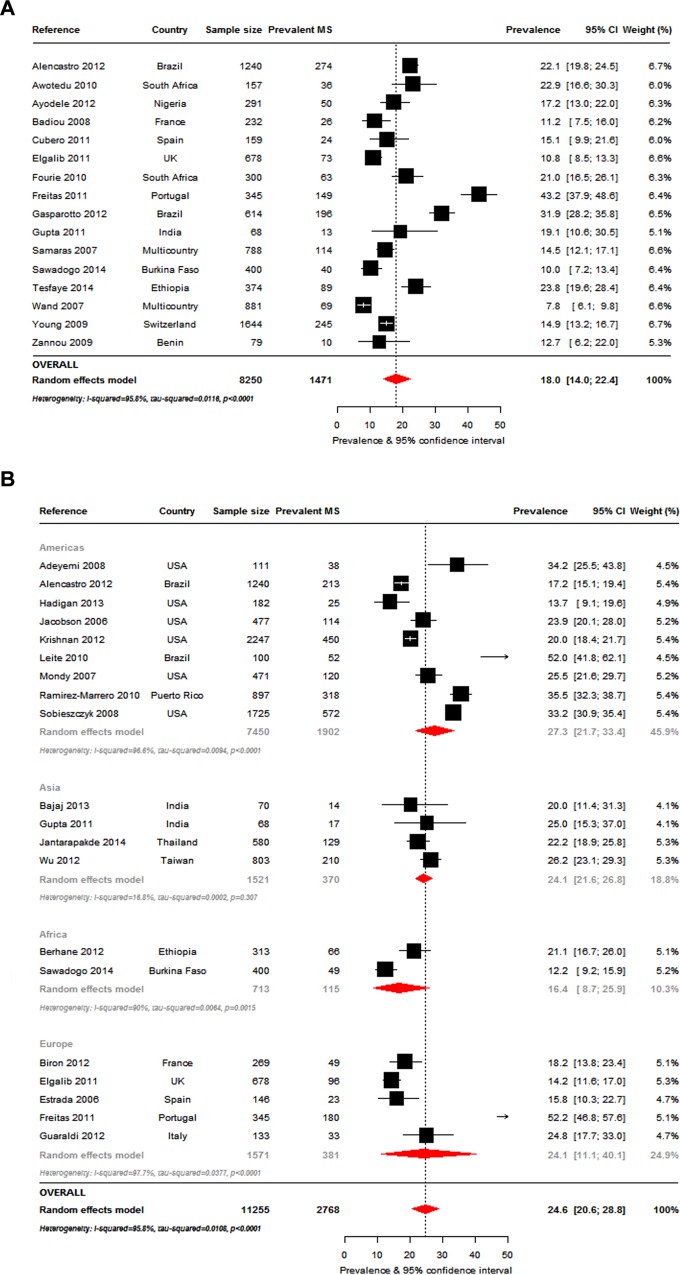
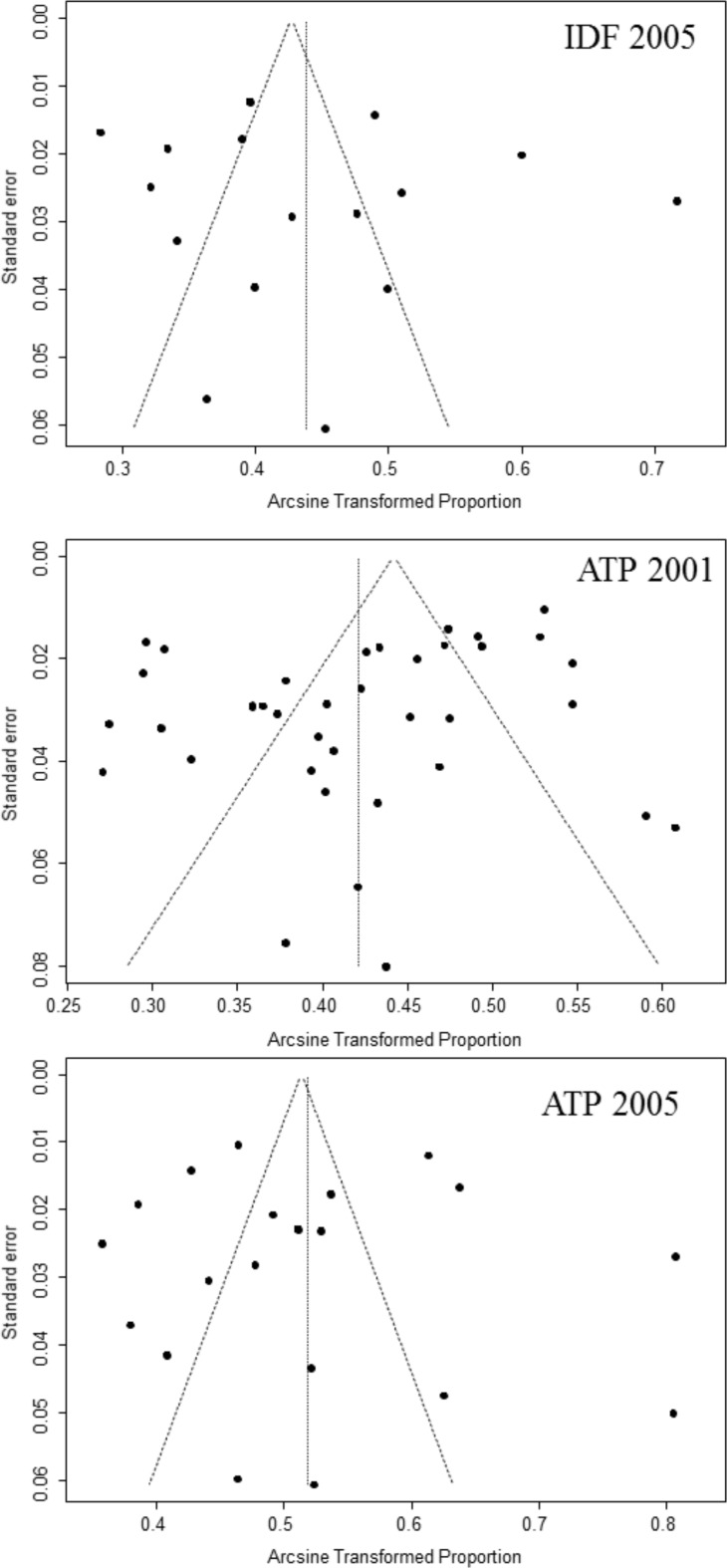
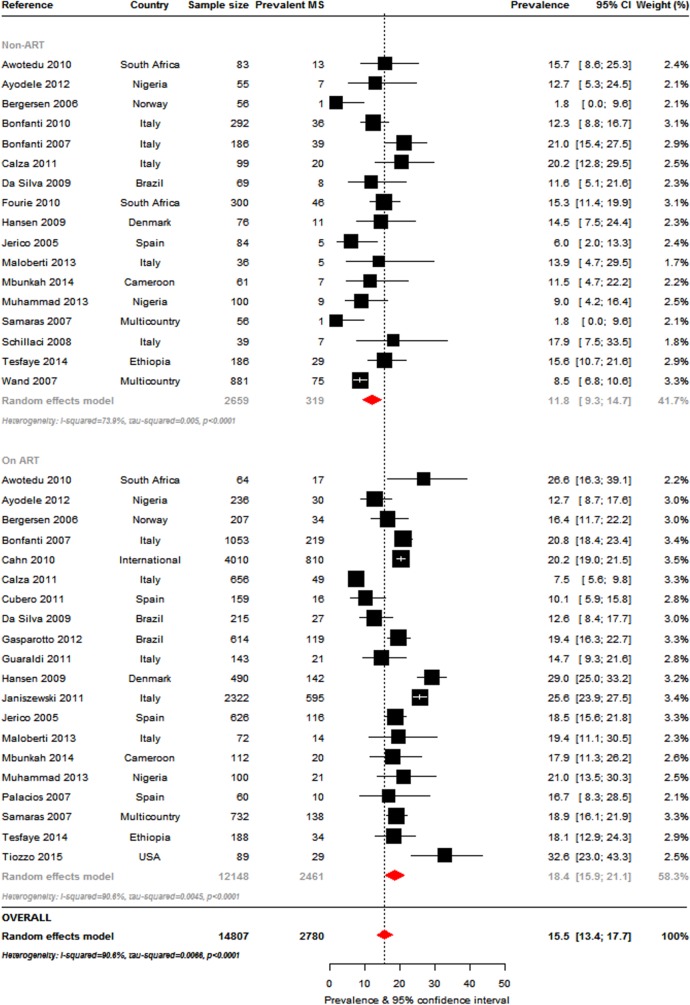
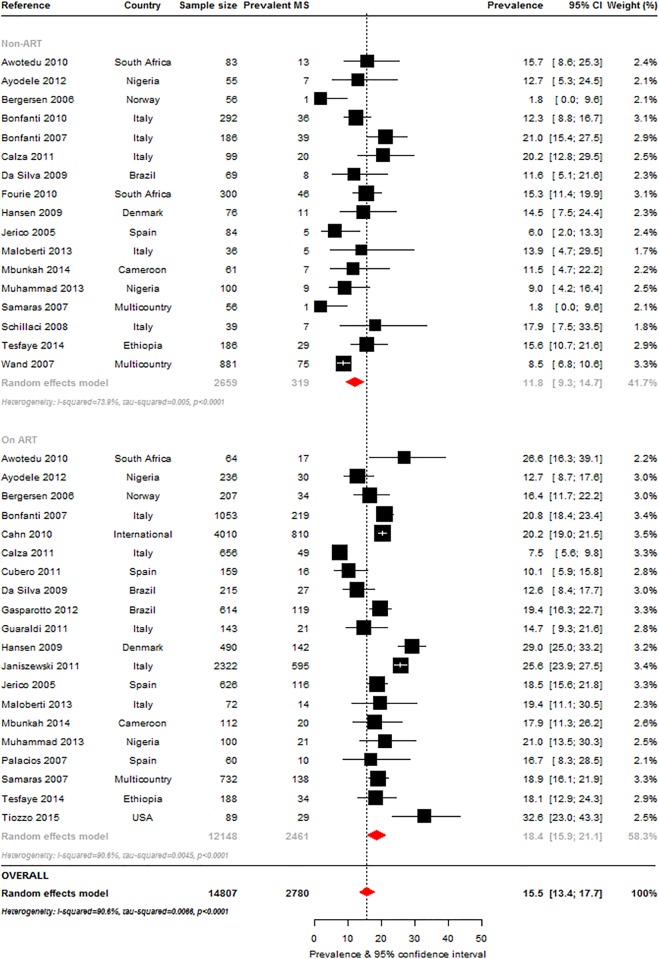
Results: A total of 65 studies across five continents comprising 55094 HIV-infected participants aged 17-73 years (median age 41 years) were included in the final meta-analysis. The overall prevalence of MS according to the following criteria were: ATPIII-2001:16.7% (95%CI: 14.6-18.8), IDF-2005: 18% (95%CI: 14.0-22.4), ATPIII-2004-2005: 24.6% (95%CI: 20.6-28.8), Modified ATPIII-2005: 27.9% (95%CI: 6.7-56.5), JIS-2009: 29.6% (95%CI: 22.9-36.8), and EGIR: 31.3% (95%CI: 26.8-36.0). By some MS criteria, the prevalence was significantly higher in women than in men (IDF-2005: 23.2% vs. 13.4, p = 0.030), in ART compared to non-ART users (ATPIII-2001: 18.4% vs. 11.8%, p = 0.001), and varied significantly by participant age, duration of HIV diagnosis, severity of infection, non-nucleoside reverse transcriptase inhibitors (NNRTIs) use and date of study publication. Across criteria, there were significant differences in MS prevalence by sub-groups such as in men, the Americas, older publications, regional studies, younger adults, smokers, ART-naïve participants, NNRTIs users, participants with shorter duration of diagnosed infection and across the spectrum of HIV severity. Substantial heterogeneities across and within criteria were not fully explained by major study characteristics, while evidence of publication bias was marginal.
Conclusions: The similar range of MS prevalence in the HIV-infected and general populations highlights the common drivers of this condition. Thus, cardio-metabolic assessments need to be routinely included in the holistic management of the HIV-infected individual. Management strategies recommended for MS in the general population will likely provide similar benefits in the HIV-infected.
Conflict of interest statement
Figures
References
-
- Murray CJ, Ortblad KF, Guinovart C, Lim SS, Wolock TM, Roberts DA, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384: 1005–1070. 10.1016/S0140-6736(14)60844-8 - DOI - PMC - PubMed
-
- Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, et al. Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. Journal of the American College of Cardiology. 2007;49: 403–414. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
