

Lung cancer incidence and mortality in National Lung Screening Trial participants who underwent low-dose CT prevalence screening: a retrospective cohort analysis of a randomised, multicentre, diagnostic screening trial
- PMID: 27009070
- PMCID: PMC5094059
- DOI: 10.1016/S1470-2045(15)00621-X
Lung cancer incidence and mortality in National Lung Screening Trial participants who underwent low-dose CT prevalence screening: a retrospective cohort analysis of a randomised, multicentre, diagnostic screening trial
Abstract
Background: Annual low-dose CT screening for lung cancer has been recommended for high-risk individuals, but the necessity of yearly low-dose CT in all eligible individuals is uncertain. This study examined rates of lung cancer in National Lung Screening Trial (NLST) participants who had a negative prevalence (initial) low-dose CT screen to explore whether less frequent screening could be justified in some lower-risk subpopulations.
Methods: We did a retrospective cohort analysis of data from the NLST, a randomised, multicentre screening trial comparing three annual low-dose CT assessments with three annual chest radiographs for the early detection of lung cancer in high-risk, eligible individuals (aged 55-74 years with at least a 30 pack-year history of cigarette smoking, and, if a former smoker, had quit within the past 15 years), recruited from US medical centres between Aug 5, 2002, and April 26, 2004. Participants were followed up for up to 5 years after their last annual screen. For the purposes of this analysis, our cohort consisted of all NLST participants who had received a low-dose CT prevalence (T0) screen. We determined the frequency, stage, histology, study year of diagnosis, and incidence of lung cancer, as well as overall and lung cancer-specific mortality, and whether lung cancers were detected as a result of screening or within 1 year of a negative screen. We also estimated the effect on mortality if the first annual (T1) screen in participants with a negative T0 screen had not been done. The NLST is registered with ClinicalTrials.gov, number NCT00047385.
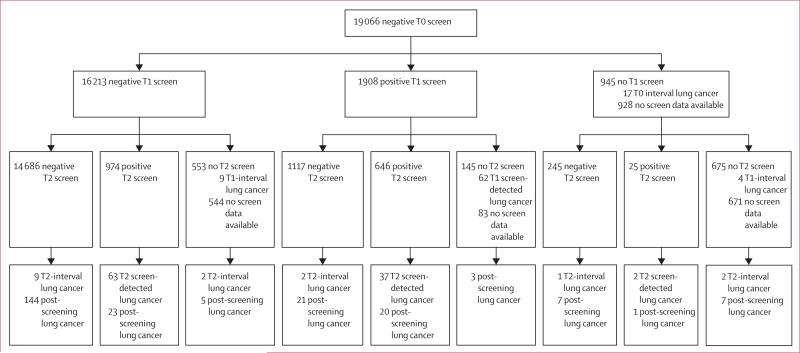
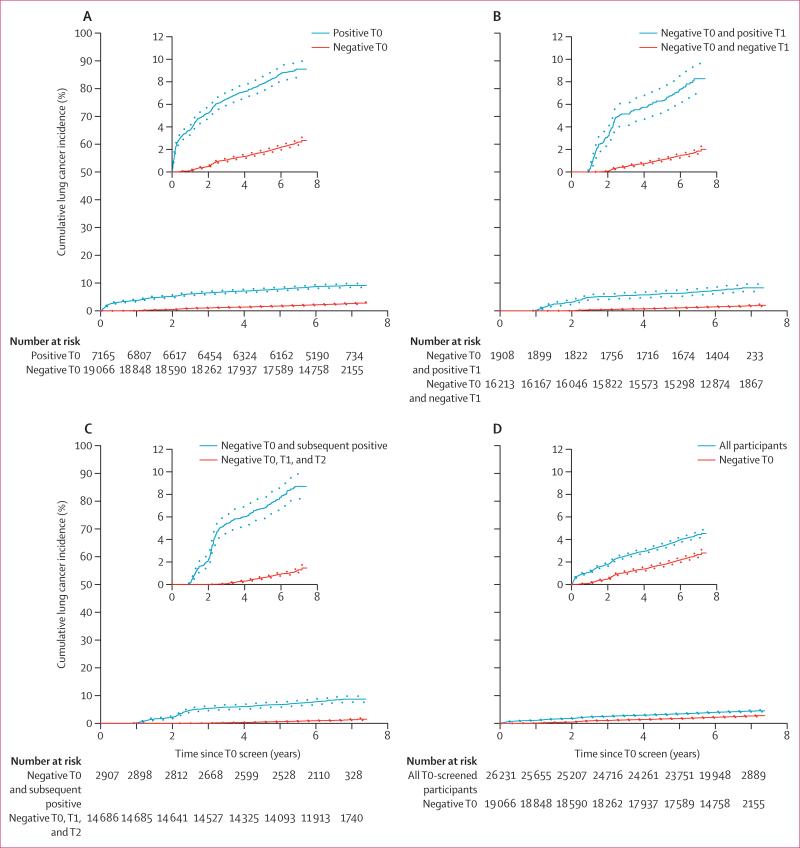
Findings: Our cohort consisted of 26 231 participants assigned to the low-dose CT screening group who had undergone their T0 screen. The 19 066 participants with a negative T0 screen had a lower incidence of lung cancer than did all 26 231 T0-screened participants (371·88 [95% CI 337·97-408·26] per 100 000 person-years vs 661·23 [622·07-702·21]) and had lower lung cancer-related mortality (185·82 [95% CI 162·17-211·93] per 100 000 person-years vs 277·20 [252·28-303·90]). The yield of lung cancer at the T1 screen among participants with a negative T0 screen was 0·34% (62 screen-detected cancers out of 18 121 screened participants), compared with a yield at the T0 screen among all T0-screened participants of 1·0% (267 of 26 231). We estimated that if the T1 screen had not been done in the T0 negative group, at most, an additional 28 participants in the T0 negative group would have died from lung cancer (a rise in mortality from 185·82 [95% CI 162·17-211·93] per 100 000 person-years to 212·14 [186·80-239·96]) over the course of the trial.
Interpretation: Participants with a negative low-dose CT prevalence screen had a lower incidence of lung cancer and lung cancer-specific mortality than did all participants who underwent a prevalence screen. Because overly frequent screening has associated harms, increasing the interval between screens in participants with a negative low-dose CT prevalence screen might be warranted.
Funding: None.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Lung cancer CT screening: is annual screening necessary?Lancet Oncol. 2016 May;17(5):543-4. doi: 10.1016/S1470-2045(16)00079-6. Epub 2016 Mar 18. Lancet Oncol. 2016. PMID: 27009071 No abstract available.
-
Lung cancer: Low-dose CT screening - determining the right interval.Nat Rev Clin Oncol. 2016 Sep;13(9):533-4. doi: 10.1038/nrclinonc.2016.106. Epub 2016 Jul 12. Nat Rev Clin Oncol. 2016. PMID: 27402578 No abstract available.
-
Reconsidering lung cancer screening: is biannual screening possible?J Thorac Dis. 2016 Sep;8(9):2372-2375. doi: 10.21037/jtd.2016.09.30. J Thorac Dis. 2016. PMID: 27746979 Free PMC article. No abstract available.
-
Annual or biennial lung cancer CT screening?J Thorac Dis. 2016 Sep;8(9):2424-2426. doi: 10.21037/jtd.2016.09.20. J Thorac Dis. 2016. PMID: 27746993 Free PMC article. No abstract available.
-
Optimizing the lung cancer screening interval: the world is waiting.J Thorac Dis. 2016 Oct;8(10):E1369-E1370. doi: 10.21037/jtd.2016.10.25. J Thorac Dis. 2016. PMID: 27867631 Free PMC article. No abstract available.
References
-
- Becker N, Motsch E, Gross ML, et al. Randomized study on early detection of lung cancer with MSCT in Germany: results of the first 3 years of follow-up after randomization. J Thorac Oncol. 2015;10:890–96. - PubMed
-
- Horeweg N, Scholten ET, de Jong PA, et al. Detection of lung cancer through low-dose CT screening (NELSON): a prespecified analysis of screening test performance and interval cancers. Lancet Oncol. 2014;15:1342–50. - PubMed
-
- Infante M, Cavuto S, Lutman FR, et al. Long-term follow-up results of the DANTE trial, a randomized study of lung cancer screening with spiral computed tomography. Am J Respir Crit Care Med. 2015;191:1166–75. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- N01 CN025512/CA/NCI NIH HHS/United States
- U01 CA080098/CA/NCI NIH HHS/United States
- N01 CN025511/CA/NCI NIH HHS/United States
- N01 CN025516/CA/NCI NIH HHS/United States
- N01 CN075022/CA/NCI NIH HHS/United States
- N02 CN063300/CA/NCI NIH HHS/United States
- UG1 CA189828/CA/NCI NIH HHS/United States
- U01 CA079778/CA/NCI NIH HHS/United States
- N01 CN025518/CA/NCI NIH HHS/United States
- N01 CN025515/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- N01 CN025514/CA/NCI NIH HHS/United States
- N01 CN025522/CA/NCI NIH HHS/United States
- N01 CN025513/CA/NCI NIH HHS/United States
- U10 CA079778/CA/NCI NIH HHS/United States
- N01 CN025524/CA/NCI NIH HHS/United States
- N01 CN025476/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
