

HIV-1 Latency and Eradication: Past, Present and Future
- PMID: 27009094
- PMCID: PMC5157928
- DOI: 10.2174/1570162x14666160324125536
HIV-1 Latency and Eradication: Past, Present and Future
Abstract
Background: It is well established that antiretroviral therapy (ART), while highly effective in controlling HIV replication, cannot eliminate virus from the body. Therefore, the majority of HIV-1-infected individuals remain at risk for developing AIDS due to persistence of infected reservoir cells serving as a source of virus re-emergence. Several reservoirs containing replication competent HIV-1 have been identified, most notably CD4+ T cells. Cells of the myeloid lineage, which are the first line of defense against pathogens and participate in HIV dissemination into sanctuary organs, also serve as cellular reservoirs of HIV-1. In latently infected resting CD4+ T cells, the integrated copies of proviral DNA remain in a dormant state, yet possess the ability to produce replication competent virus after cellular activation. Studies have demonstrated that modification of chromatin structure plays a role in establishing persistence, in part suggesting that latency is, controlled epigenetically.
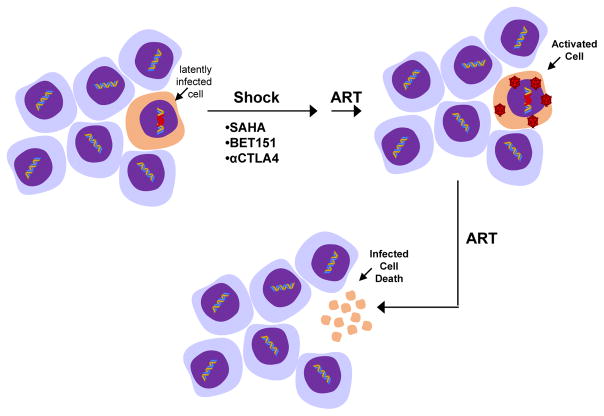
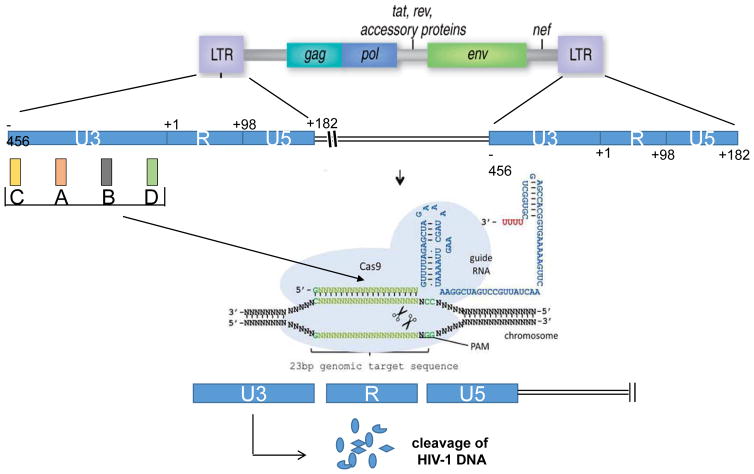
Conclusion: Current efforts to eradicate HIV-1 from this cell population focus primarily on a "shock and kill" approach through cellular reactivation to trigger elimination of virus producing cells by cytolysis or host immune responses. However, studies revealed several limitations to this approach that require more investigation to assess its clinical application. Recent advances in gene editing technology prompted use of this approach for inactivating integrated proviral DNA in the genome of latently infected cells. This technology, which requires a detailed understanding of the viral genetics and robust delivery, may serve as a powerful strategy to eliminate the latent reservoir in the host leading to a sterile cure of AIDS.
Conflict of interest statement
Conflict of Interests The authors have no conflict of interest to declare
Figures
References
-
- Lewden C, Chene G, Morlat P, et al. HIV-infected adults with a CD4 cell count greater than 500 cells/mm3 on long-term combination antiretroviral therapy reach same mortality rates as the general population. J Acquir Immune Defic Syndr. 2007;46:72–7. - PubMed
-
- Hearps AC, Martin GE, Rajasuriar R, et al. Inflammatory co-morbidities in HIV+ individuals: learning lessons from healthy ageing. Curr HIV/AIDS Rep. 2014;11:20–34. - PubMed
-
- Samaras K. Prevalence and pathogenesis of diabetes mellitus in HIV-1 infection treated with combined antiretroviral therapy. J Acquir Immune Defic Syndr. 2009 Apr 15;50(5):499–505. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous