

Does Antihypertensive Drug Class Affect Day-to-Day Variability of Self-Measured Home Blood Pressure? The HOMED-BP Study
- PMID: 27009620
- PMCID: PMC4943272
- DOI: 10.1161/JAHA.115.002995
Does Antihypertensive Drug Class Affect Day-to-Day Variability of Self-Measured Home Blood Pressure? The HOMED-BP Study
Abstract
Background: Recent literature suggests that blood pressure variability (BPV) predicts outcome beyond blood pressure level (BPL) and that antihypertensive drug classes differentially influence BPV. We compared calcium channel blockers, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockade for effects on changes in self-measured home BPL and BPV and for their prognostic significance in newly treated hypertensive patients.
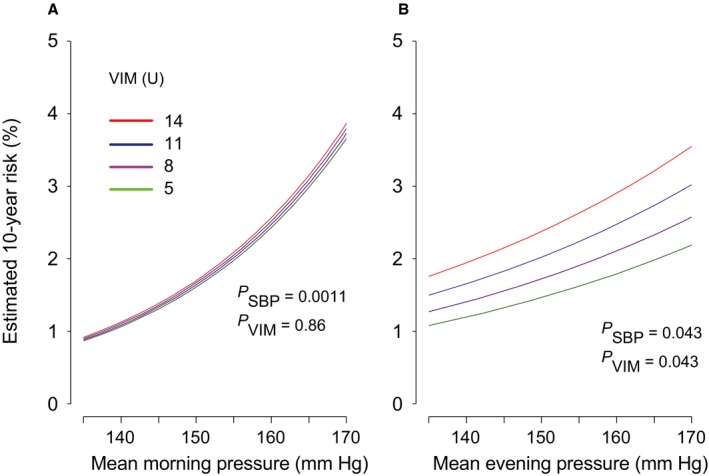
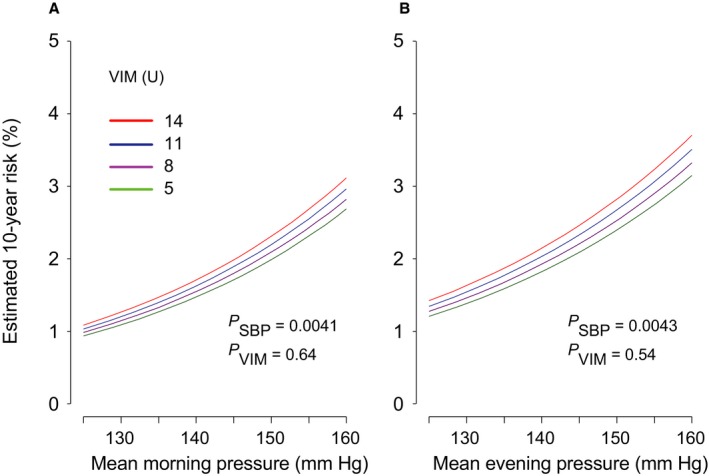
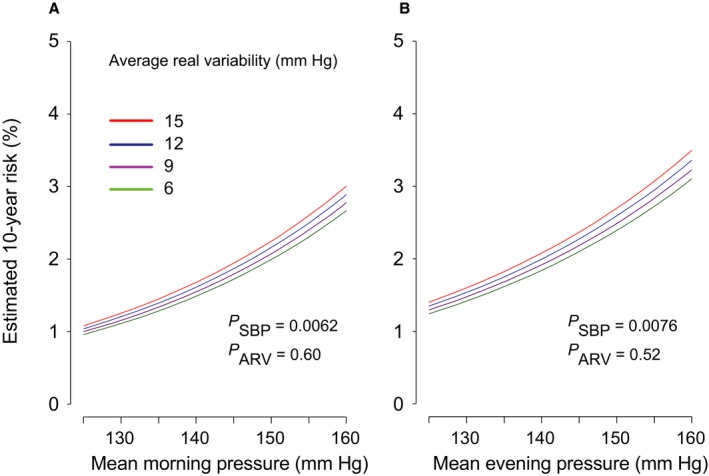
Methods and results: We enrolled 2484 patients randomly allocated to first-line treatment with a calcium channel blocker (n=833), an angiotensin-converting enzyme inhibitor (n=821), or angiotensin receptor blockade (n=830). Home blood pressures in the morning and evening were measured for 5 days off treatment before randomization and for 5 days after 2 to 4 weeks of randomized drug treatment. We assessed BPL and BPV changes as estimated by variability independent of the mean and compared cardiovascular outcomes. Home BPL response in each group was significant (P≤0.0001) but small in the angiotensin-converting enzyme inhibitor group (systolic/diastolic: 4.6/2.8 mm Hg) compared with the groups treated with a calcium channel blocker (systolic/diastolic: 8.3/3.9 mm Hg) and angiotensin receptor blockade (systolic/diastolic: 8.2/4.5 mm Hg). In multivariable adjusted analyses, changes in home variability independent of the mean did not differ among the 3 drug classes (P≥0.054). Evening variability independent of the mean before treatment significantly predicted hard cardiovascular events independent of the corresponding home BPL (P≤0.022), whereas BPV did not predict any cardiovascular outcome based on the morning measurement (P≥0.056). Home BPV captured after monotherapy had no predictive power for cardiovascular outcome (P≥0.22).
Conclusions: Self-measured home evening BPV estimated by variability independent of the mean had prognostic significance, whereas antihypertensive drug classes had no significant impact on BPV changes. Home BPL should remain the primary focus for risk stratification and treatment.
Clinical trial registration: URL: http://www.umin.ac.jp/ctr/index.htm. Unique identifier: C000000137.
Keywords: antihypertensive drugs; blood pressure variability; cardiovascular outcomes; home blood pressure; morning and evening self‐measurement.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures


Similar articles
-
Combined effect of angiotensin II receptor blocker and either a calcium channel blocker or diuretic on day-by-day variability of home blood pressure: the Japan Combined Treatment With Olmesartan and a Calcium-Channel Blocker Versus Olmesartan and Diuretics Randomized Efficacy Study.Hypertension. 2012 Jun;59(6):1132-8. doi: 10.1161/HYPERTENSIONAHA.111.189217. Epub 2012 Apr 30. Hypertension. 2012. PMID: 22547439 Clinical Trial.
-
Cardiovascular outcomes in the first trial of antihypertensive therapy guided by self-measured home blood pressure.Hypertens Res. 2012 Nov;35(11):1102-10. doi: 10.1038/hr.2012.125. Epub 2012 Aug 16. Hypertens Res. 2012. PMID: 22895063 Clinical Trial.
-
Antihypertensive drug classes have different effects on short-term blood pressure variability in essential hypertension.Hypertens Res. 2014 Jun;37(6):585-90. doi: 10.1038/hr.2014.33. Epub 2014 Mar 27. Hypertens Res. 2014. PMID: 24671016
-
Effect of antihypertensive treatment on 24-h blood pressure variability: pooled individual data analysis of ambulatory blood pressure monitoring studies based on olmesartan mono or combination treatment.J Hypertens. 2018 Apr;36(4):720-733. doi: 10.1097/HJH.0000000000001608. J Hypertens. 2018. PMID: 29045341 Free PMC article. Review.
-
Effects of renin-angiotensin system inhibition on end-organ protection: can we do better?Clin Ther. 2007 Sep;29(9):1803-24. doi: 10.1016/j.clinthera.2007.09.019. Clin Ther. 2007. PMID: 18035185 Review.
Cited by
-
Effect of Azilsartan on Day-to-Day Variability in Home Blood Pressure: A Prospective Multicenter Clinical Trial.J Clin Med Res. 2017 Jul;9(7):618-623. doi: 10.14740/jocmr3050w. Epub 2017 May 22. J Clin Med Res. 2017. PMID: 28611863 Free PMC article.
-
Age-Related Trends in Home Blood Pressure, Home Pulse Rate, and Day-to-Day Blood Pressure and Pulse Rate Variability Based on Longitudinal Cohort Data: The Ohasama Study.J Am Heart Assoc. 2019 Aug 6;8(15):e012121. doi: 10.1161/JAHA.119.012121. Epub 2019 Jul 23. J Am Heart Assoc. 2019. PMID: 31333055 Free PMC article.
-
The effects of increasing calcium channel blocker dose vs. adding a diuretic to treatment regimens for patients with uncontrolled hypertension.Hypertens Res. 2017 Oct 5;40(10):892-898. doi: 10.1038/hr.2017.56. Epub 2017 Apr 27. Hypertens Res. 2017. PMID: 28446804 Clinical Trial.
-
Blood Pressure Variability and Therapeutic Implications in Hypertension and Cardiovascular Diseases.High Blood Press Cardiovasc Prev. 2019 Oct;26(5):353-359. doi: 10.1007/s40292-019-00339-z. Epub 2019 Sep 26. High Blood Press Cardiovasc Prev. 2019. PMID: 31559570 Free PMC article. Review.
-
Left ventricular hypertrophy by electrocardiogram as a predictor of success in home blood pressure control: HOMED-BP study.Hypertens Res. 2017 May;40(5):504-510. doi: 10.1038/hr.2016.176. Epub 2017 Jan 12. Hypertens Res. 2017. PMID: 28077858 Clinical Trial.
References
-
- Staessen JA, Thijs L, Ohkubo T, Kikuya M, Richart T, Boggia J, Adiyaman A, Dechering DG, Kuznetsova T, Thien T, de Leeuw P, Imai Y, O'Brien E, Parati G. Thirty years of research on diagnostic and therapeutic thresholds for the self‐measured blood pressure at home. Blood Press Monit. 2008;13:352–365. - PubMed
-
- Pickering TG, Miller NH, Ogedegbe G, Krakoff LR, Artinian NT, Goff D. Call to action on use and reimbursement for home blood pressure monitoring: a joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension. 2008;52:10–29. - PMC - PubMed
-
- Rothwell PM, Howard SC, Dolan E, O'Brien E, Dobson JE, Dahlof B, Sever PS, Poulter NR. Prognostic significance of visit‐to‐visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010;375:895–905. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
