

Physical fitness training for stroke patients
- PMID: 27010219
- PMCID: PMC6464717
- DOI: 10.1002/14651858.CD003316.pub6
Physical fitness training for stroke patients
Update in
-
Physical fitness training for stroke patients.Cochrane Database Syst Rev. 2020 Mar 20;3(3):CD003316. doi: 10.1002/14651858.CD003316.pub7. Cochrane Database Syst Rev. 2020. PMID: 32196635 Free PMC article.
Abstract
Background: Levels of physical fitness are low after stroke. It is unknown whether improving physical fitness after stroke reduces disability.
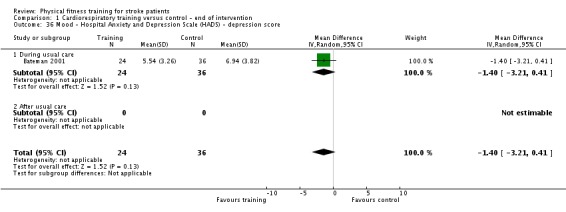
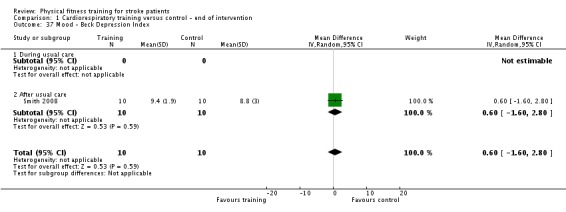
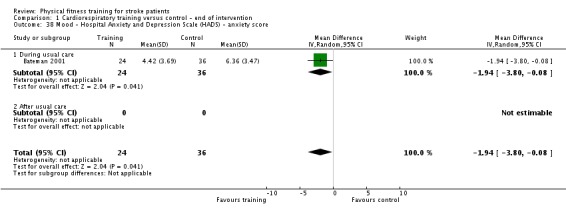
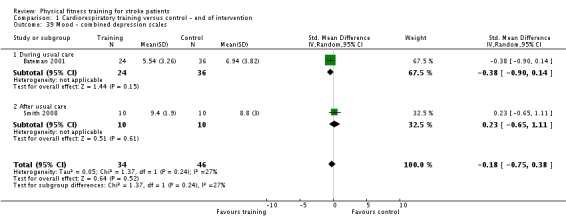
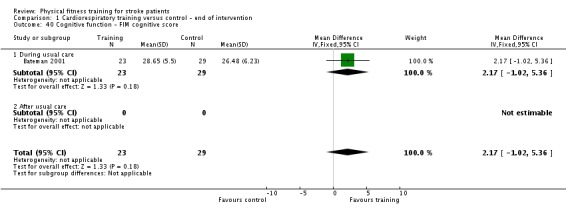
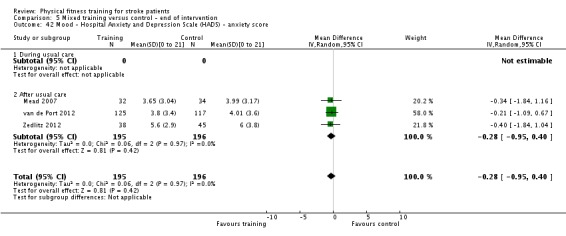
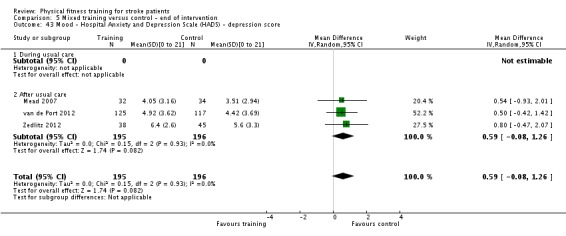
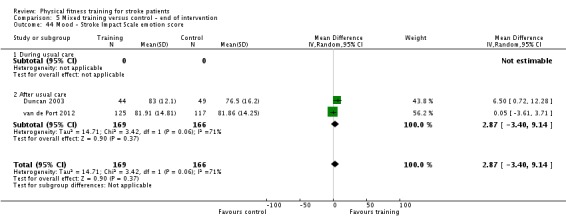
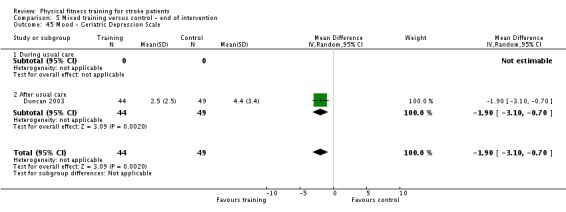
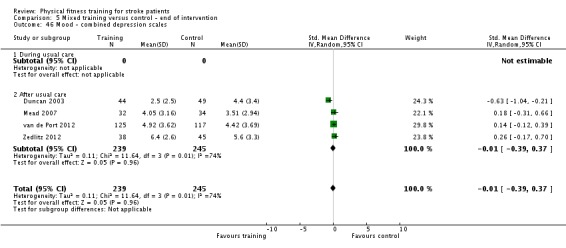
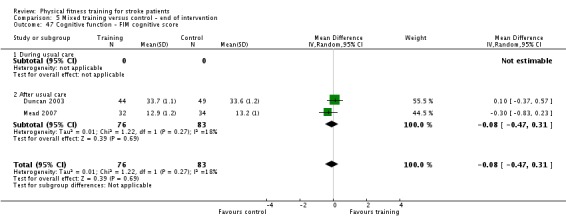
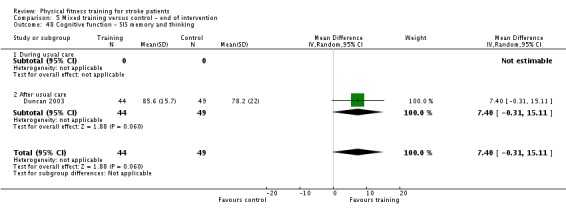
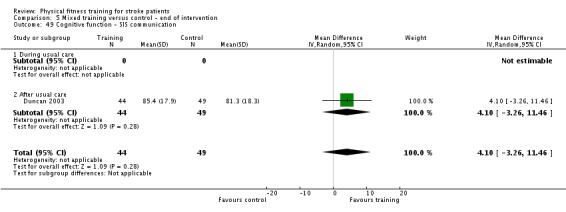
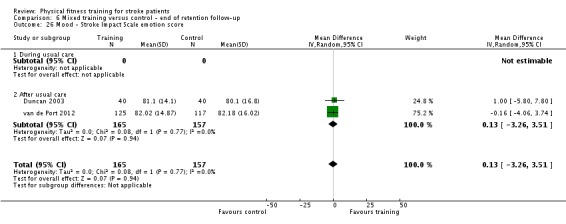
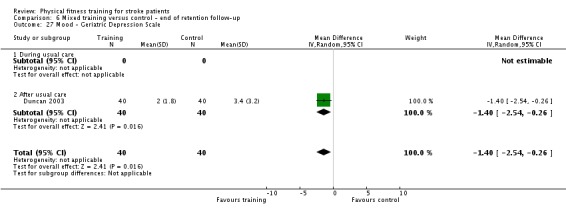
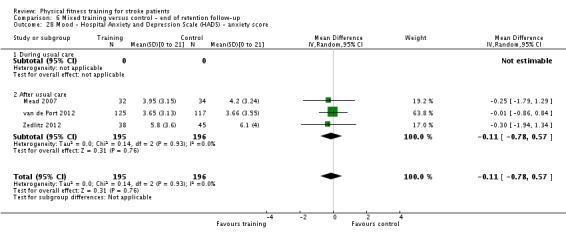
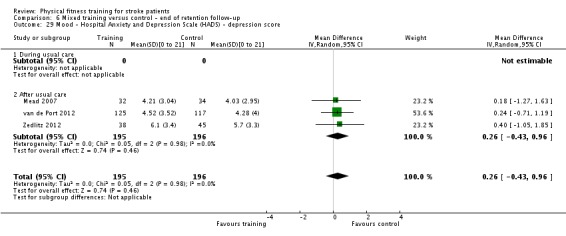
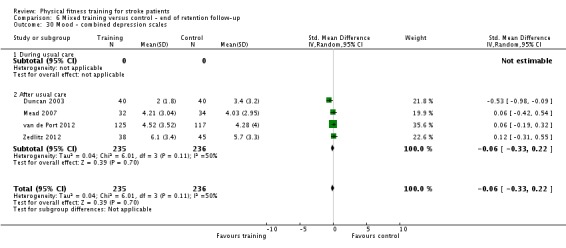
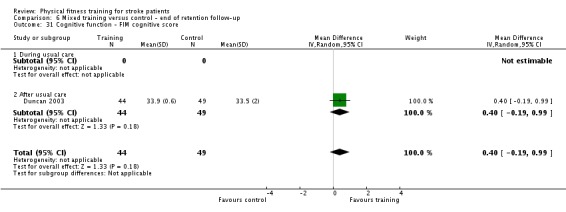
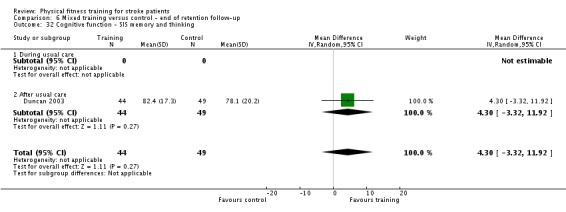
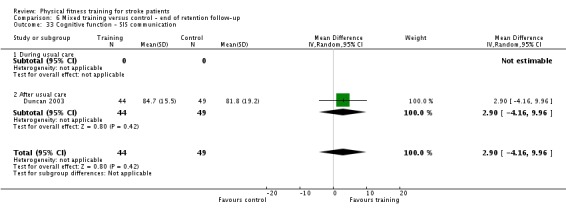
Objectives: To determine whether fitness training after stroke reduces death, dependence, and disability and to assess the effects of training with regard to adverse events, risk factors, physical fitness, mobility, physical function, quality of life, mood, and cognitive function. Interventions to improve cognitive function have attracted increased attention after being identified as the highest rated research priority for life after stroke. Therefore we have added this class of outcomes to this updated review.
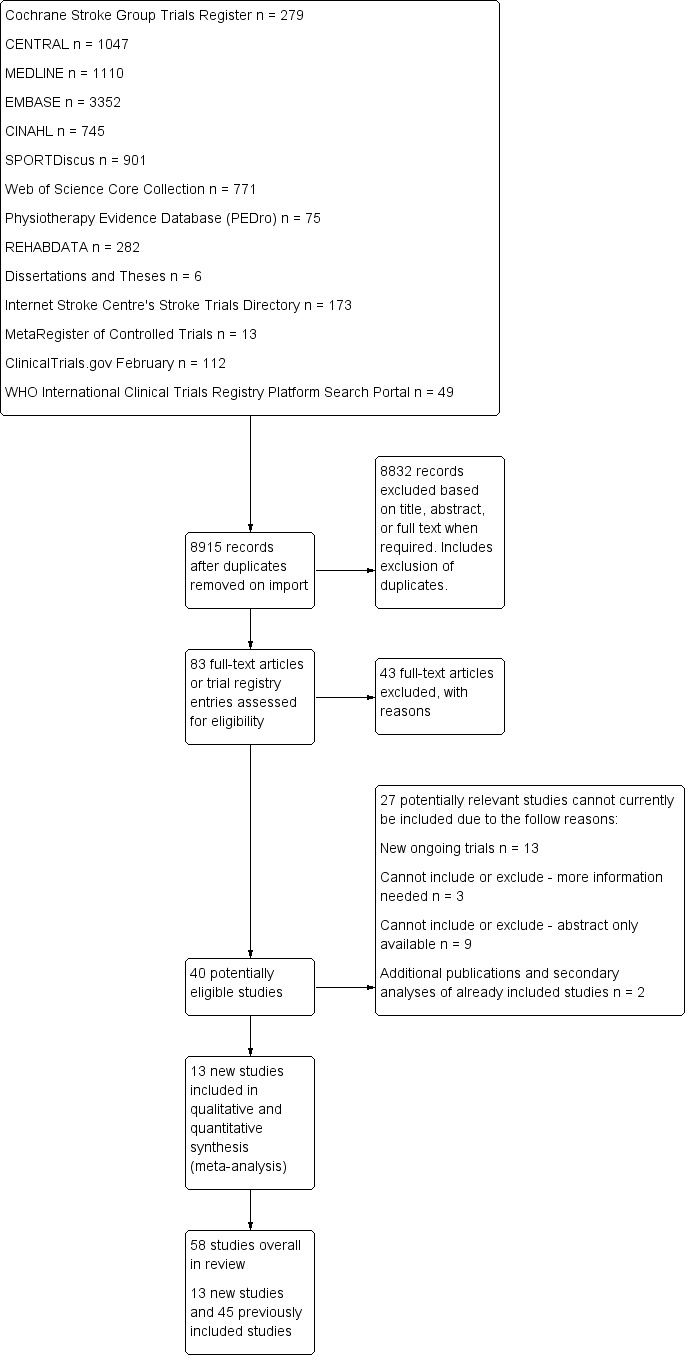
Search methods: We searched the Cochrane Stroke Group Trials Register (last searched February 2015), the Cochrane Central Register of Controlled Trials (CENTRAL 2015, Issue 1: searched February 2015), MEDLINE (1966 to February 2015), EMBASE (1980 to February 2015), CINAHL (1982 to February 2015), SPORTDiscus (1949 to February 2015), and five additional databases (February 2015). We also searched ongoing trials registers, handsearched relevant journals and conference proceedings, screened reference lists, and contacted experts in the field.
Selection criteria: Randomised trials comparing either cardiorespiratory training or resistance training, or both (mixed training), with usual care, no intervention, or a non-exercise intervention in stroke survivors.
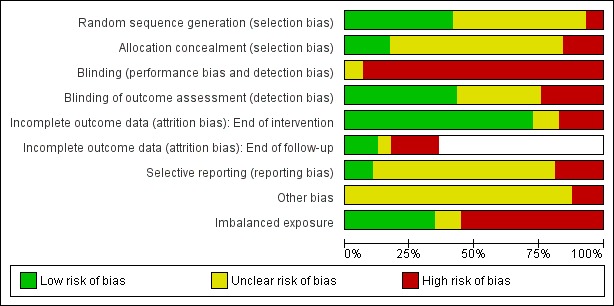
Data collection and analysis: Two review authors independently selected trials, assessed quality and risk of bias, and extracted data. We analysed data using random-effects meta-analyses. Diverse outcome measures limited the intended analyses.
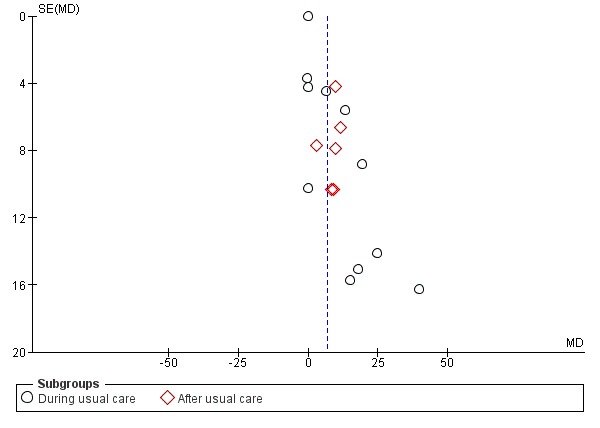
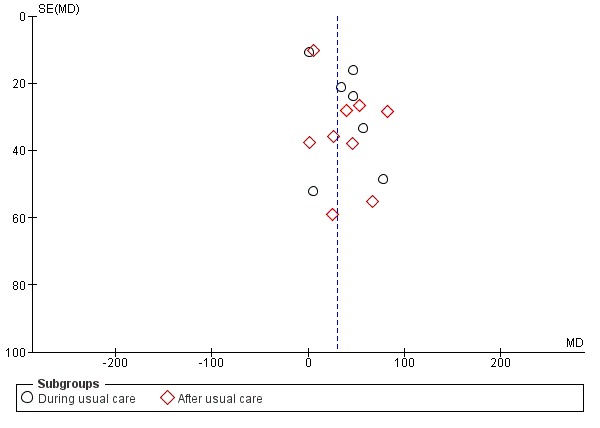
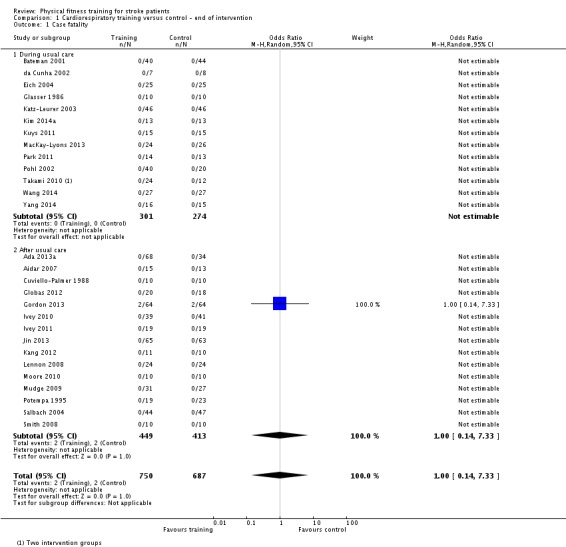
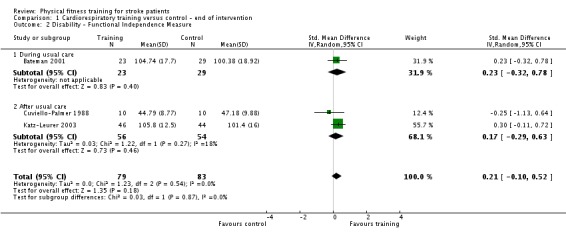
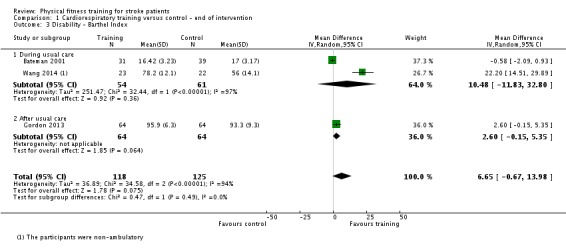
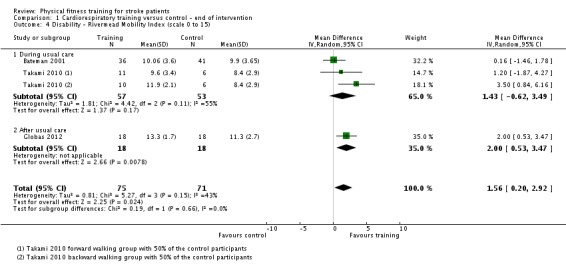
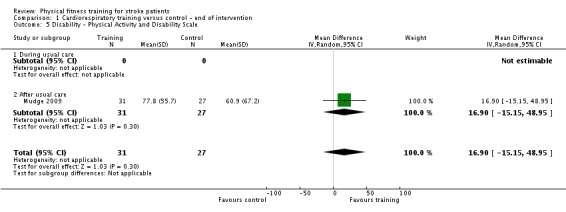
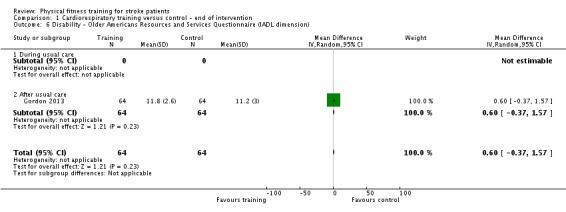
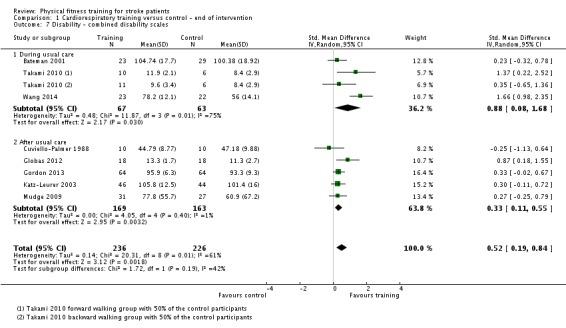
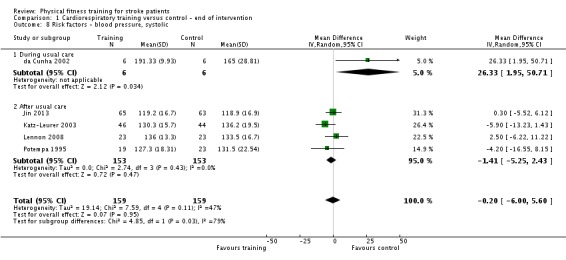
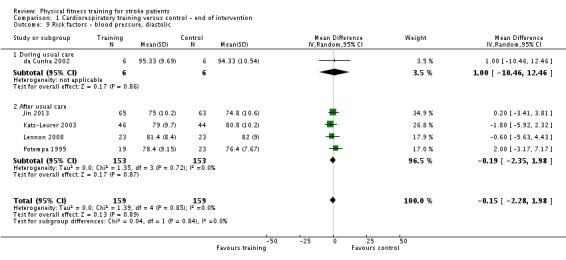
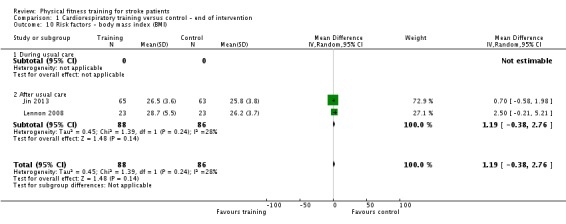
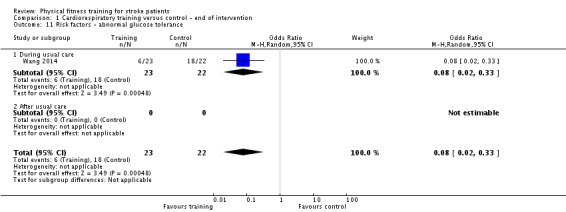
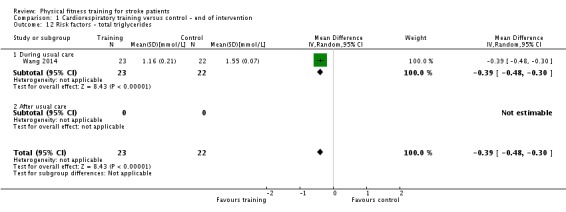
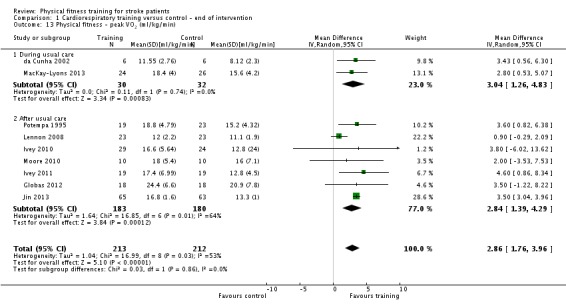
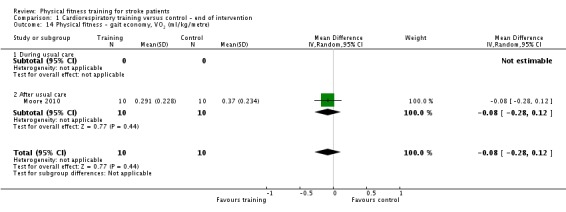
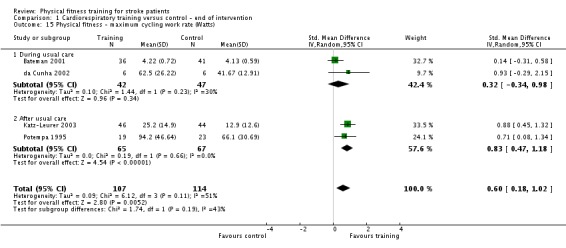
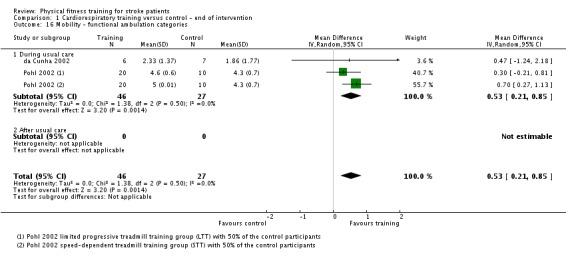
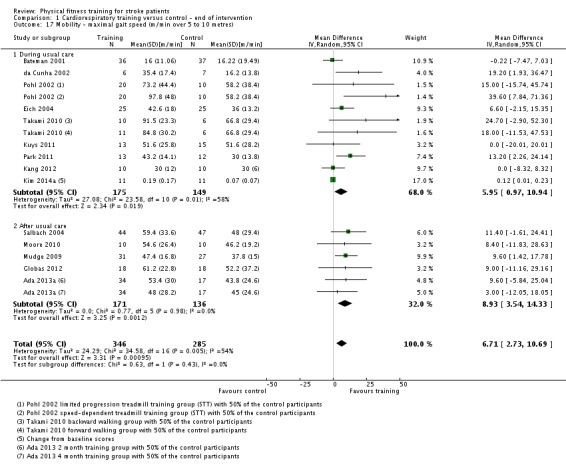
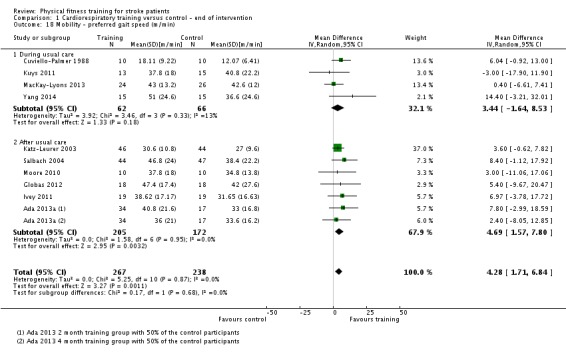
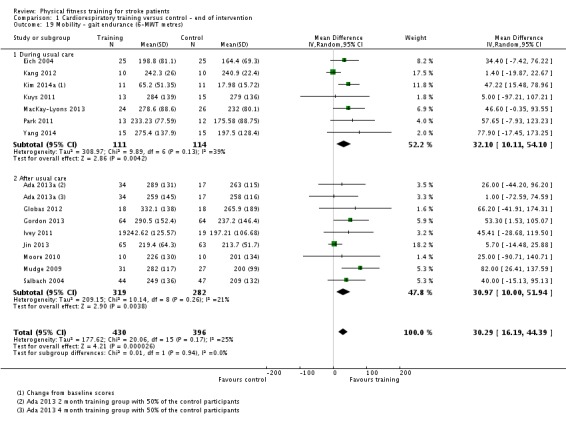
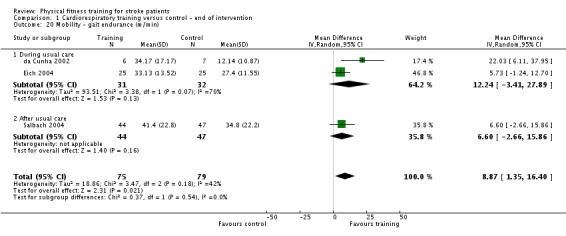
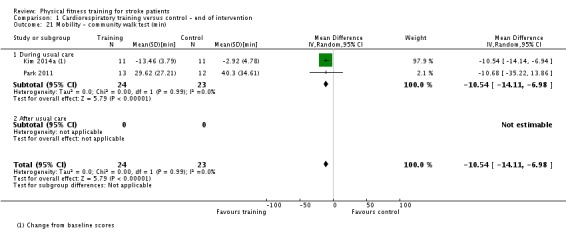
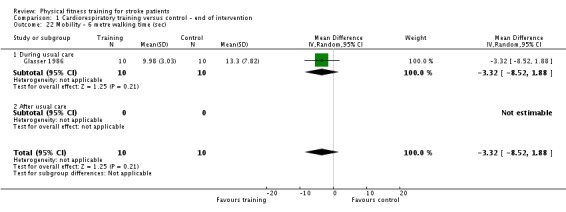
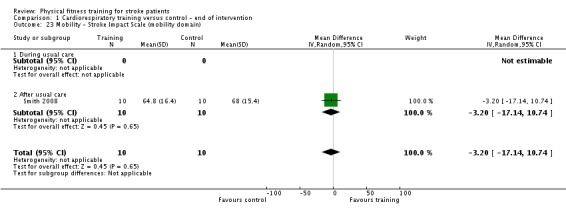
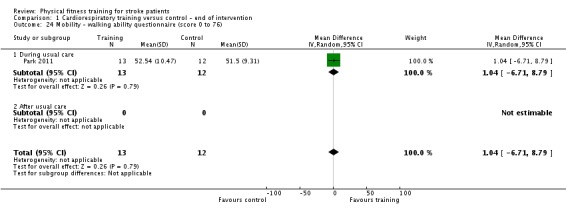
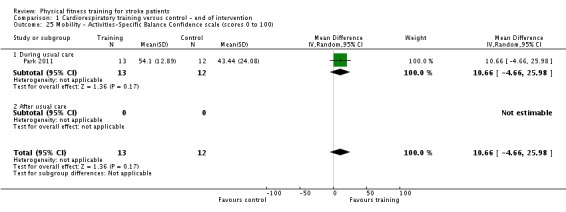
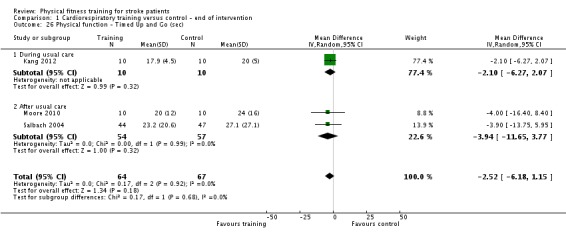
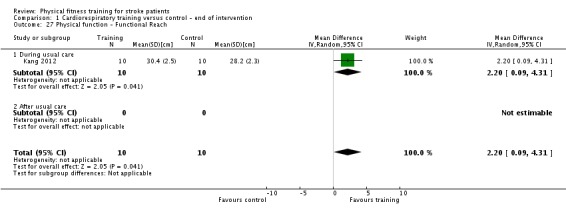
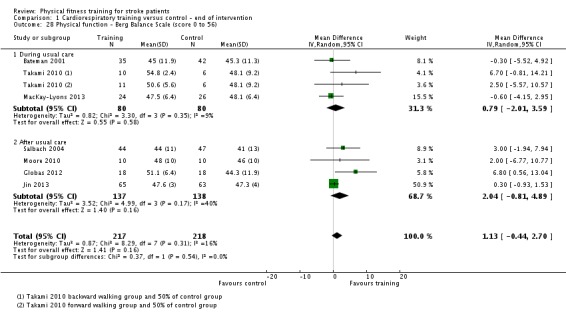
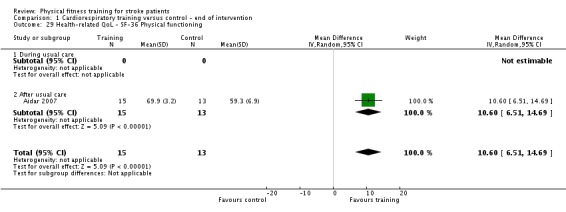
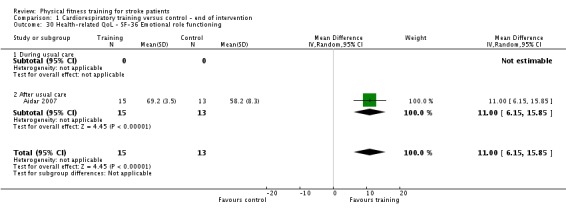
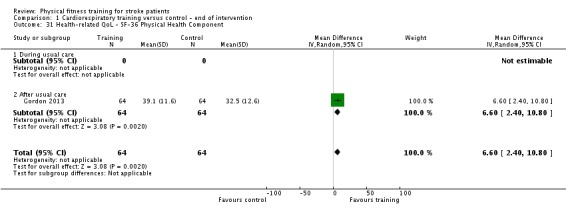
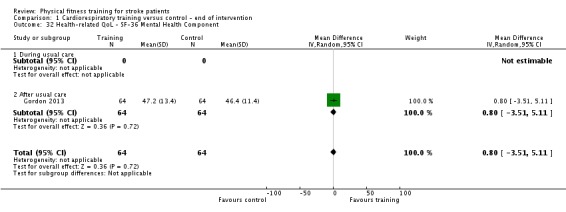
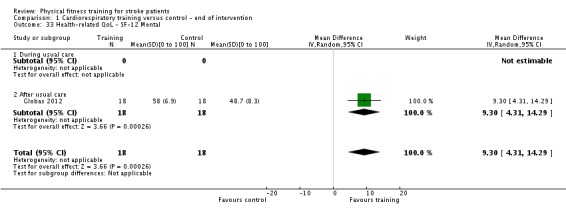
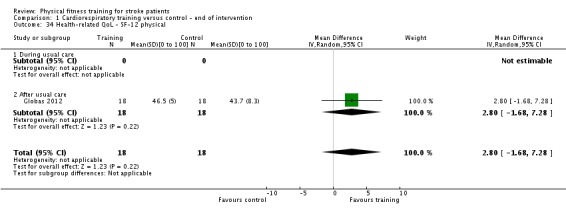
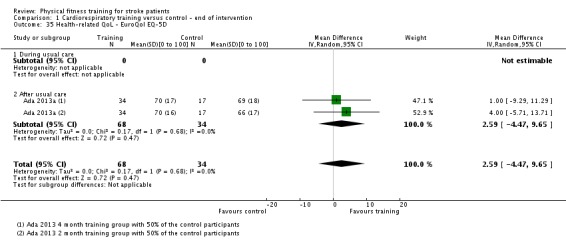
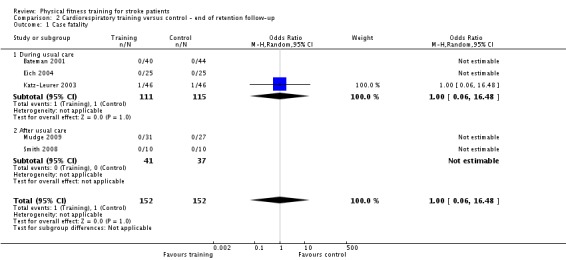
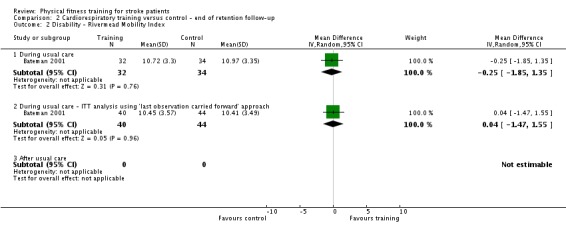
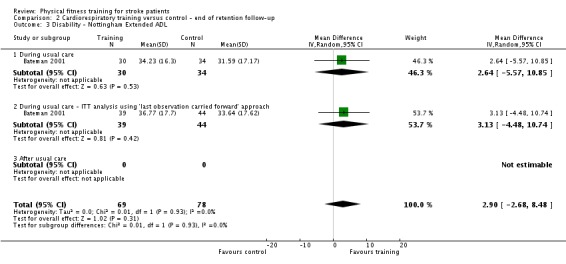
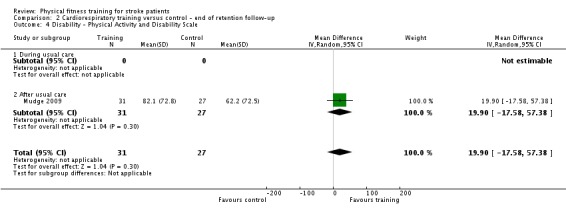
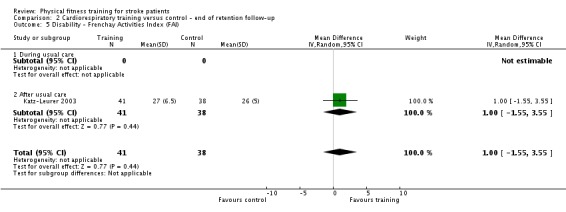
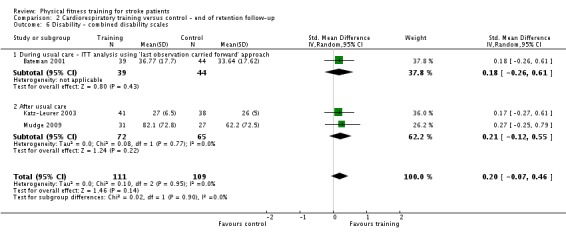
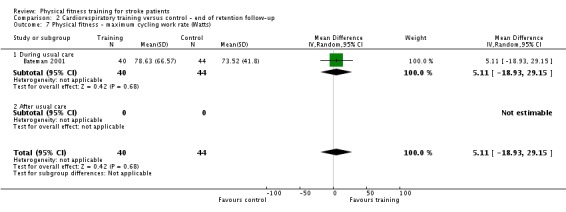
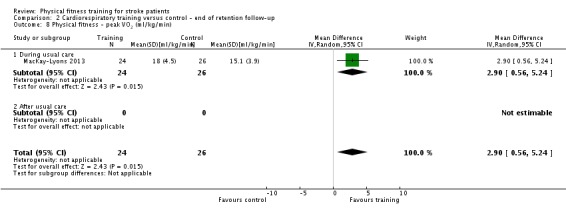
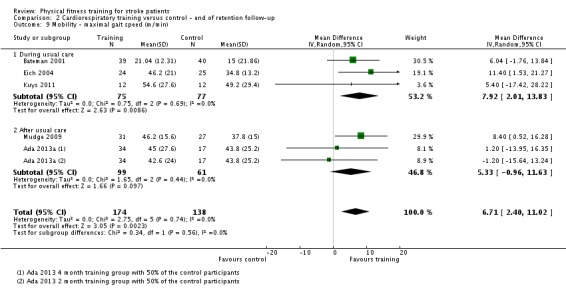
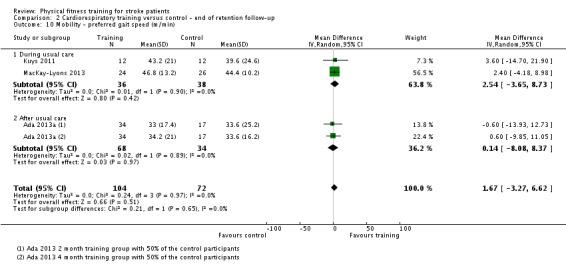
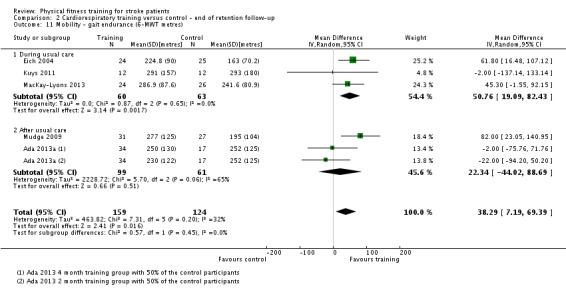
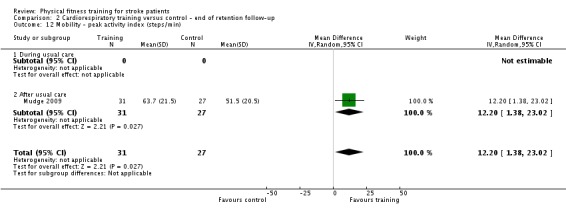
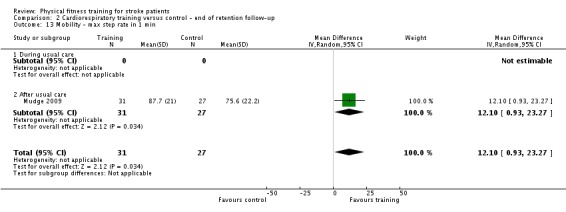
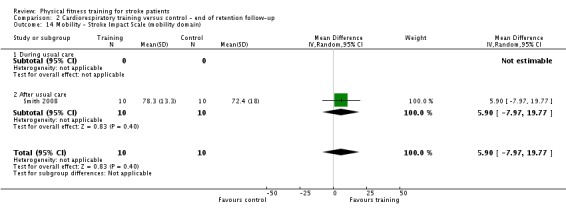
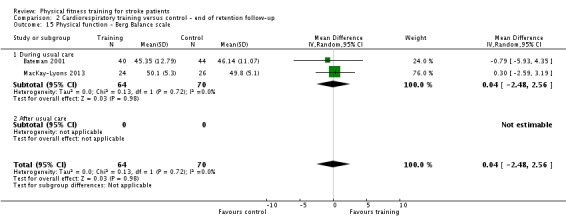
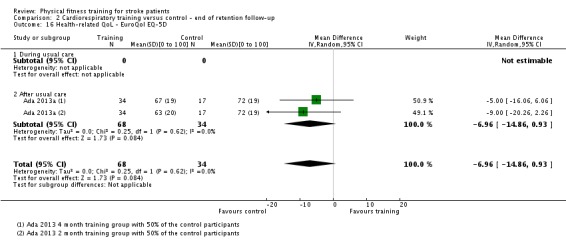
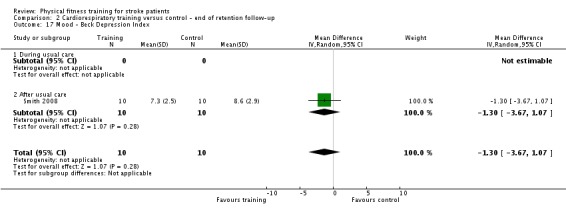
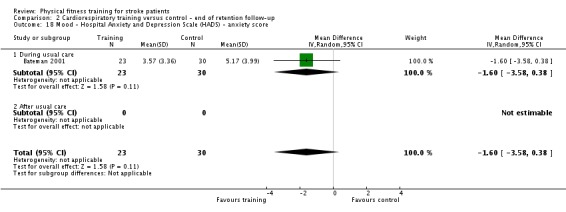
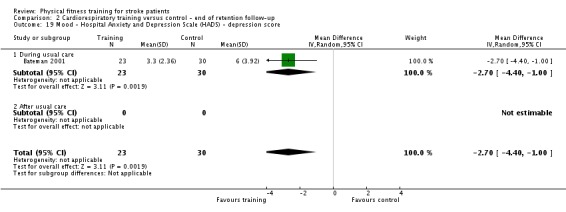
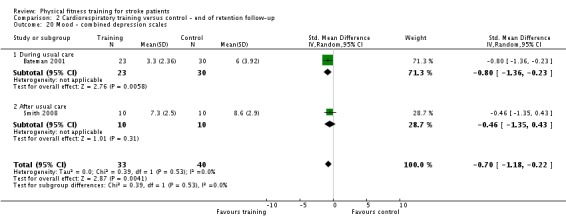
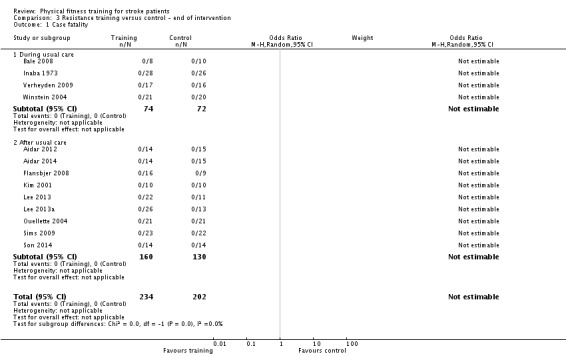
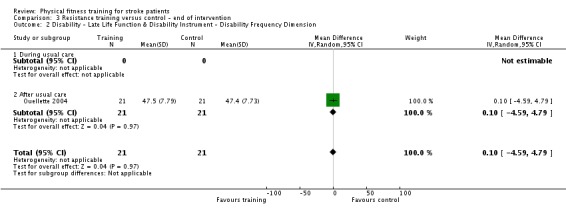
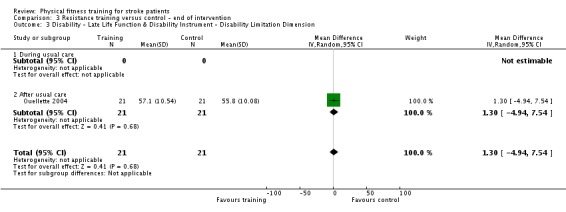
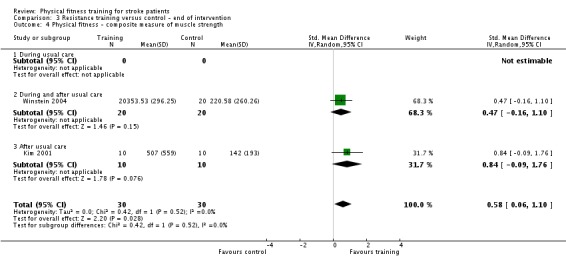
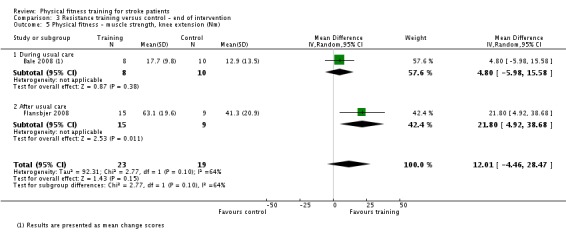
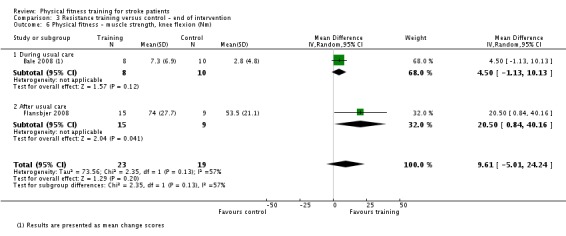
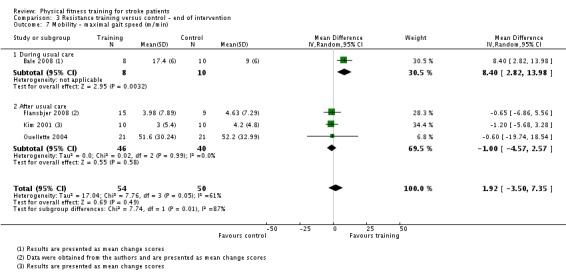
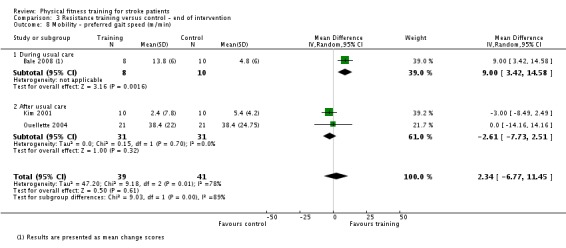
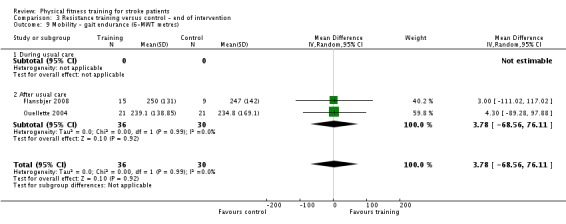
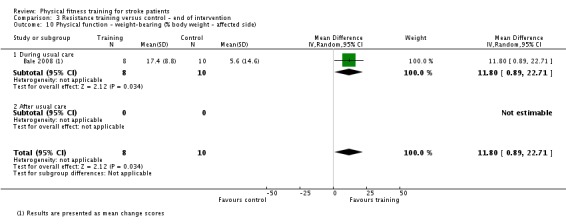
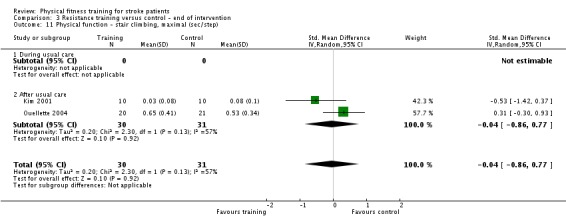
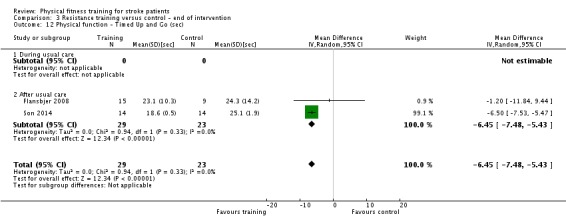
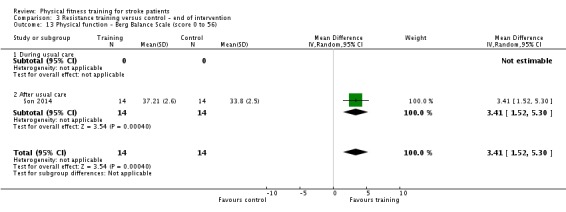
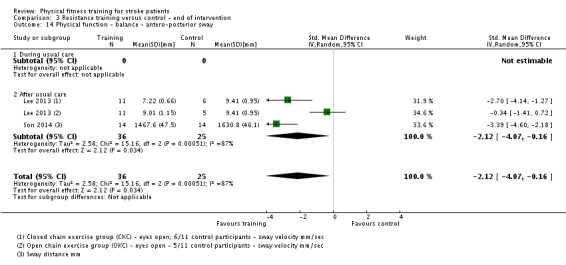
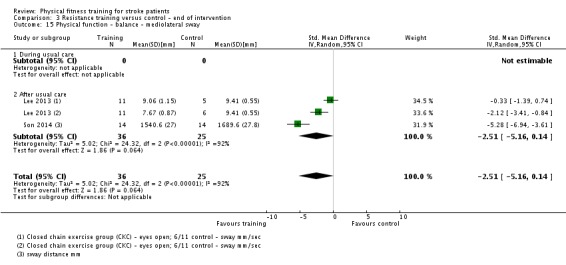
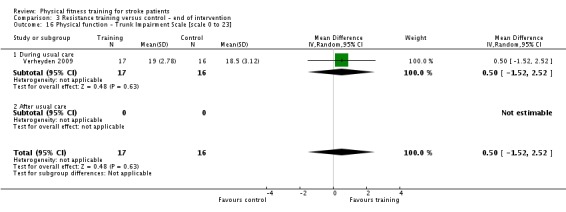
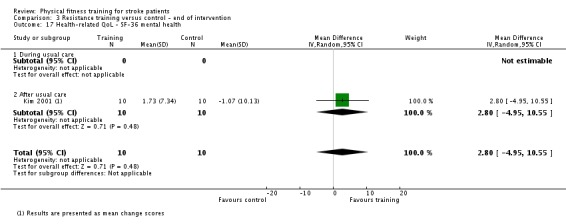
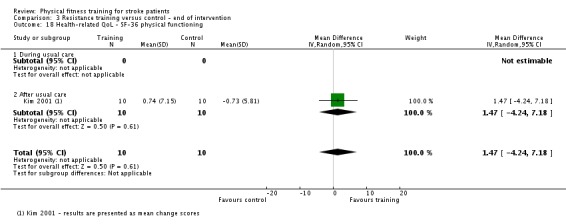
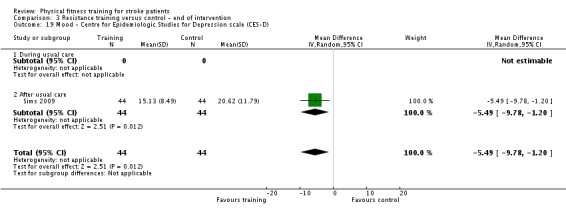
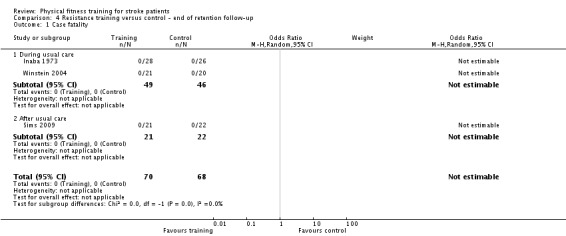
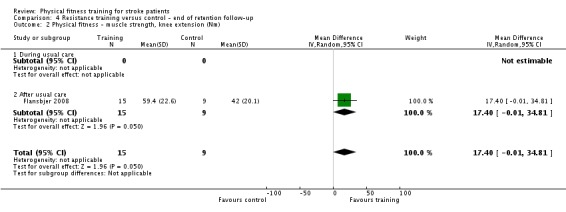
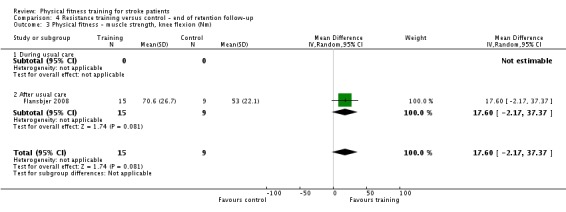
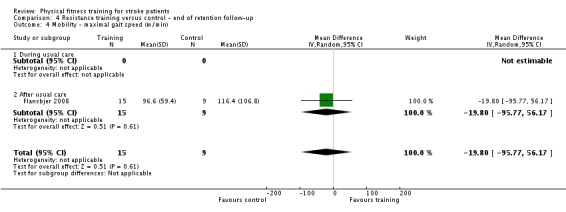
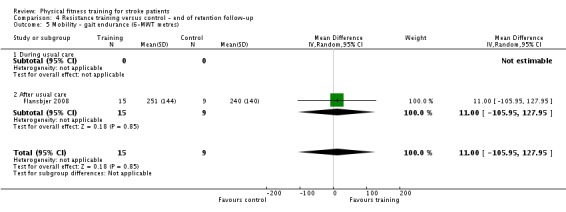
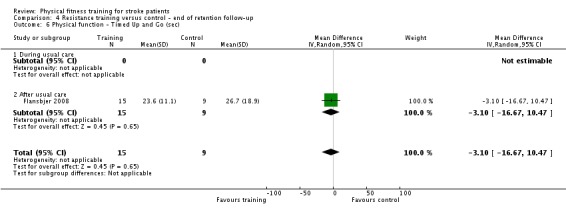
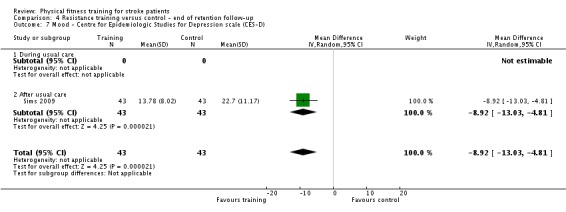
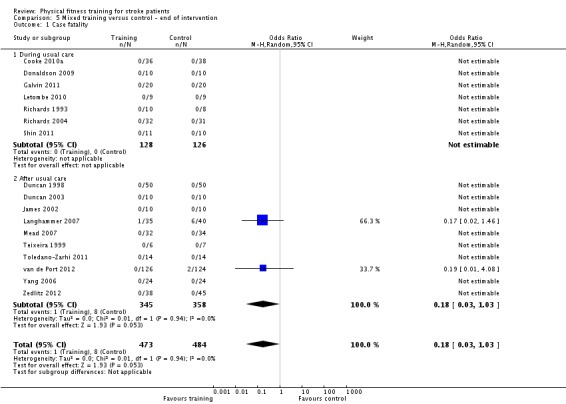
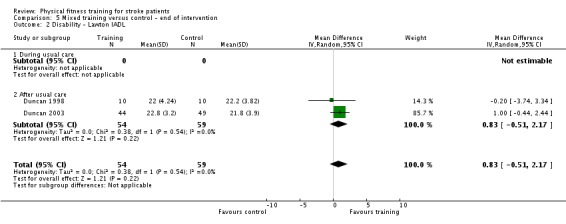
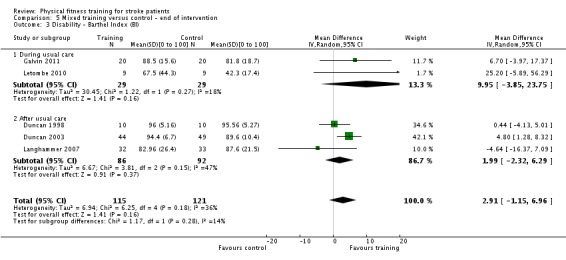
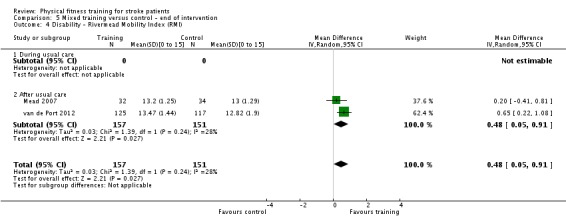
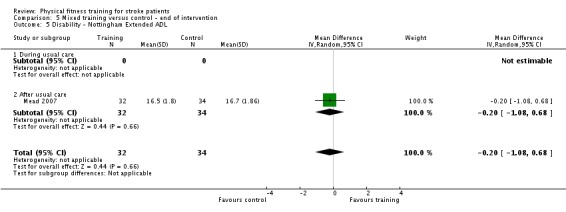
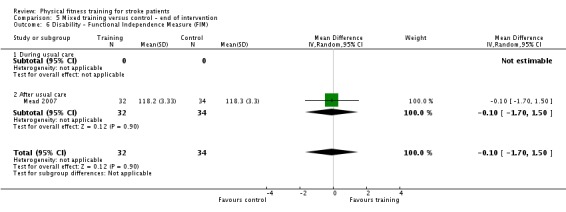
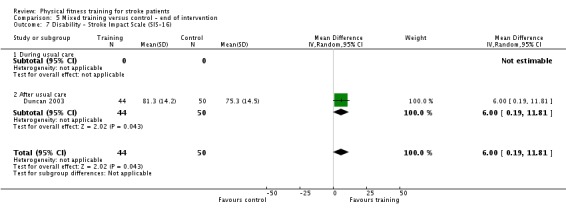
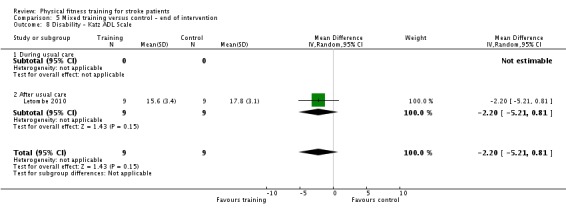
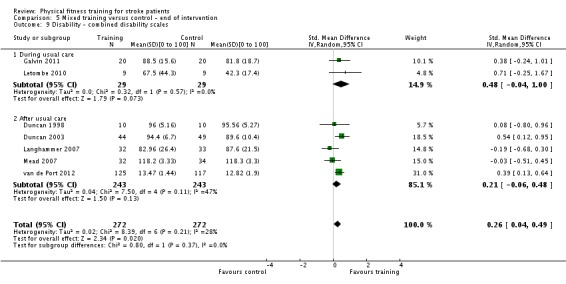
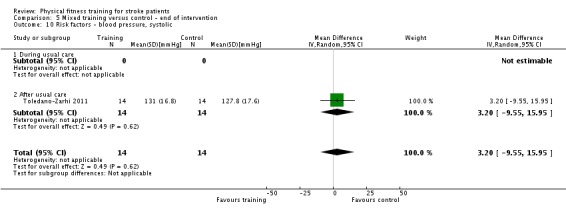
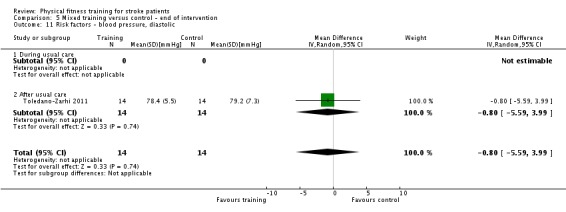
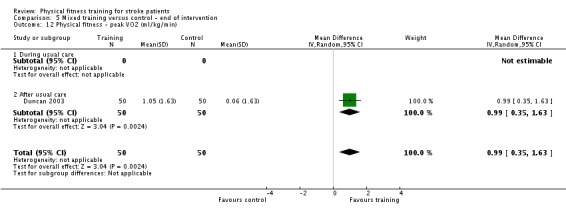
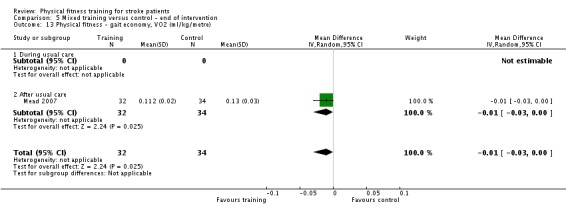
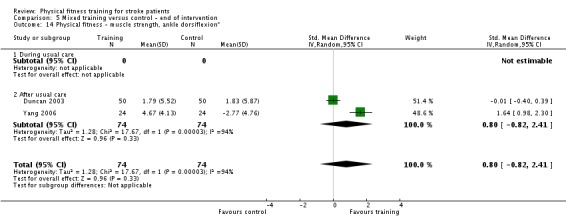
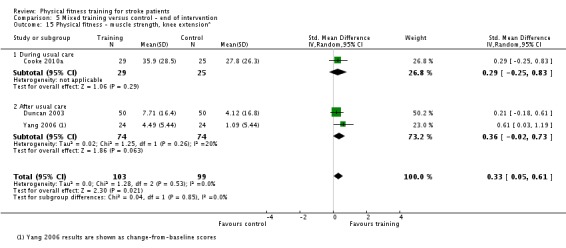
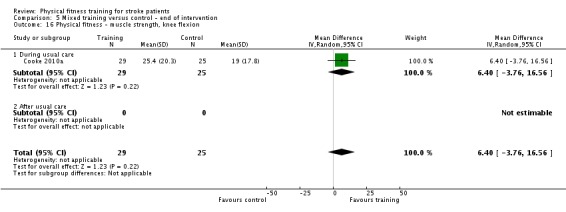
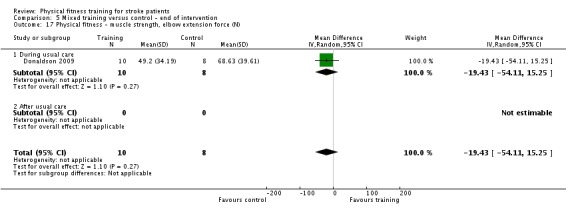
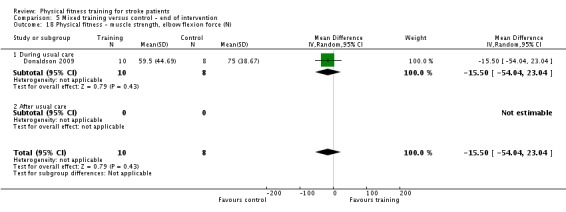
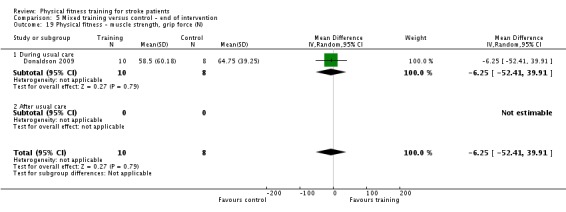
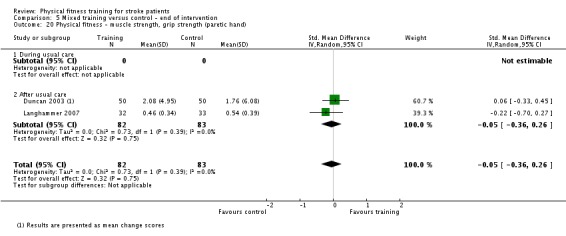
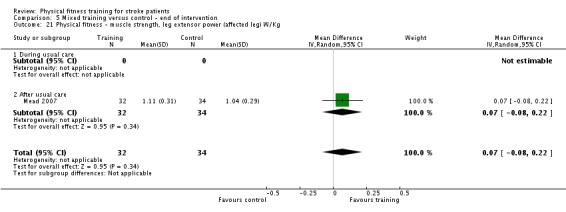
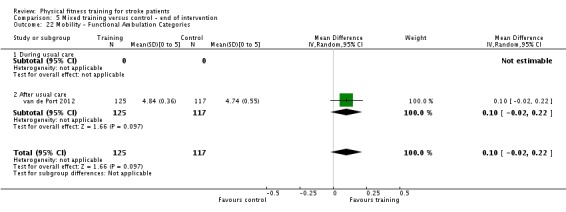
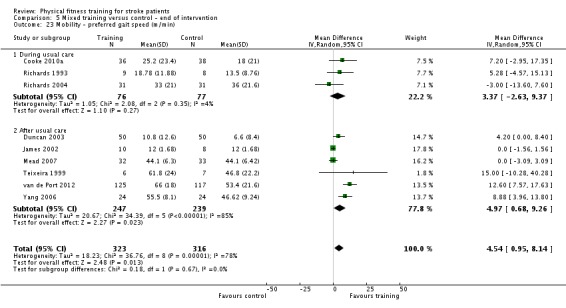
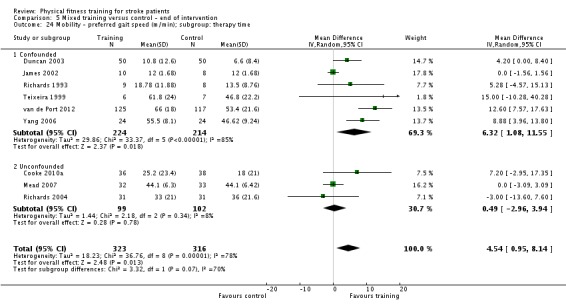
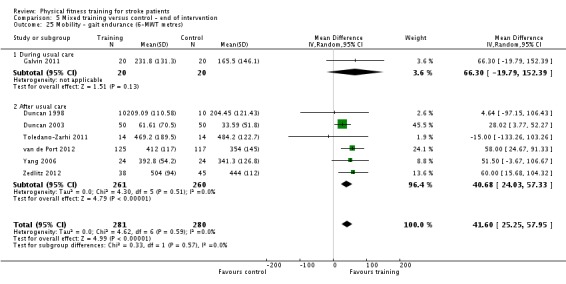
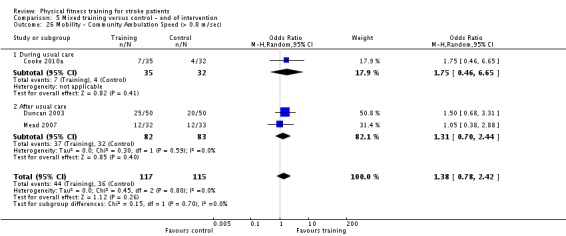
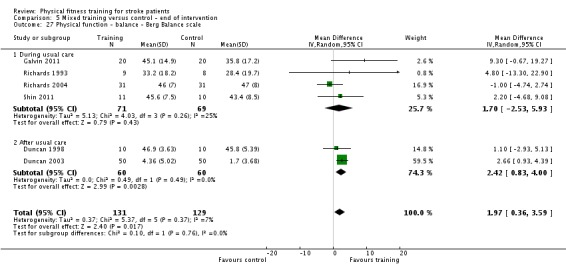
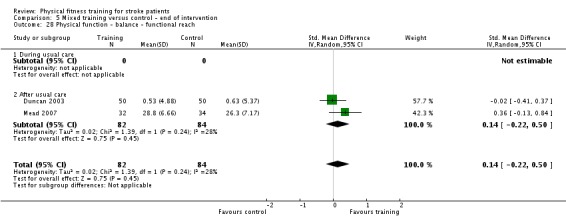
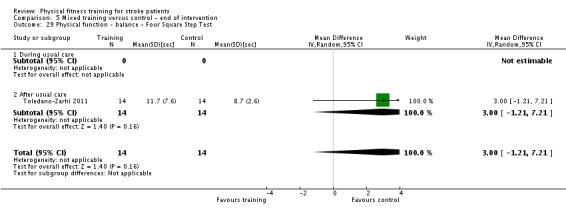
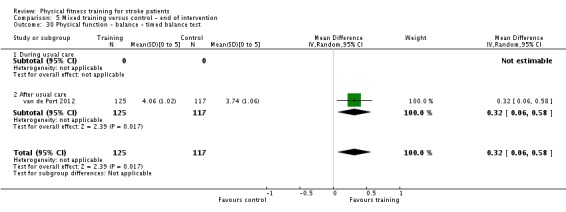
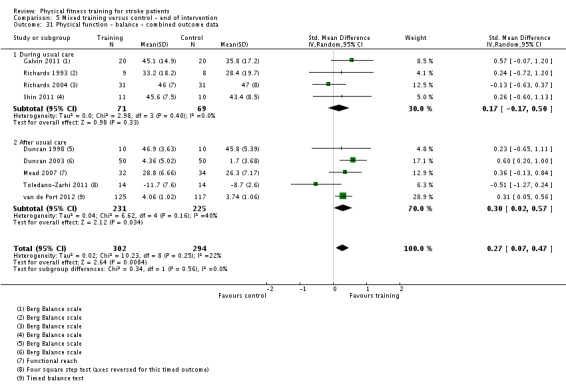
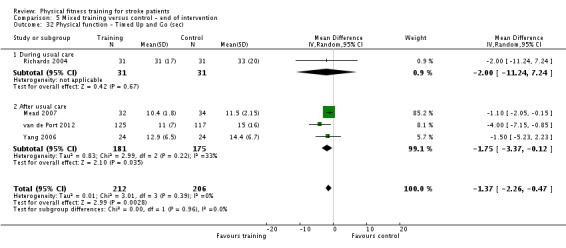
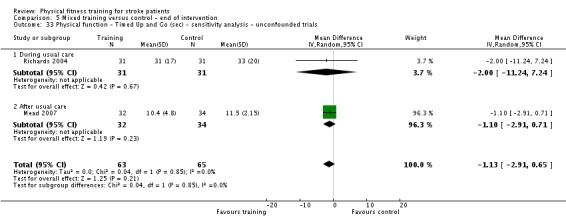
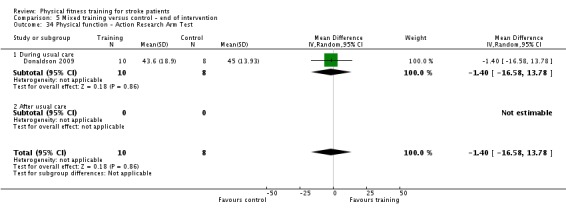
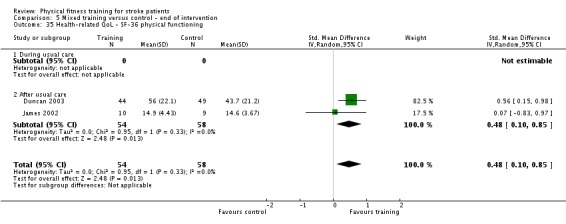
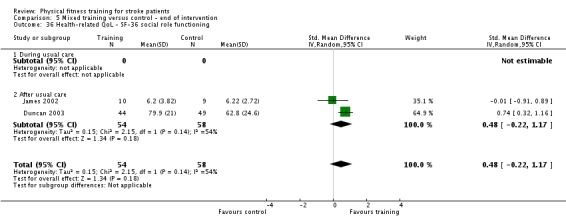
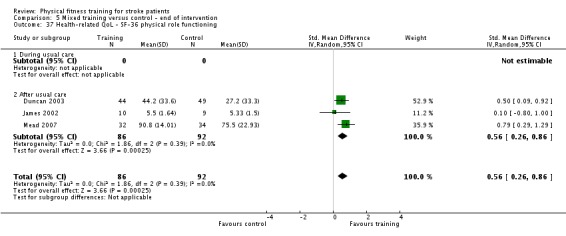
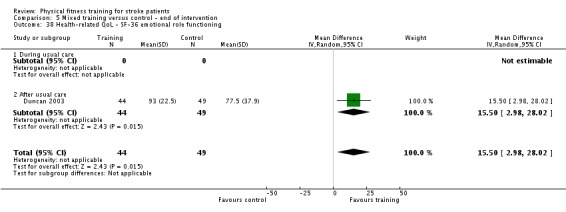
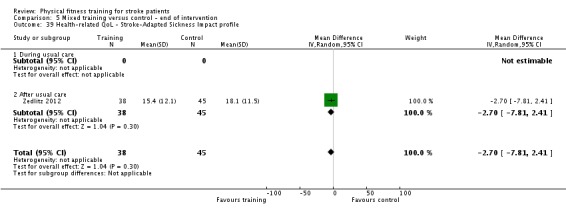
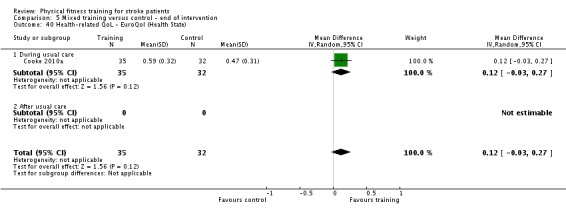
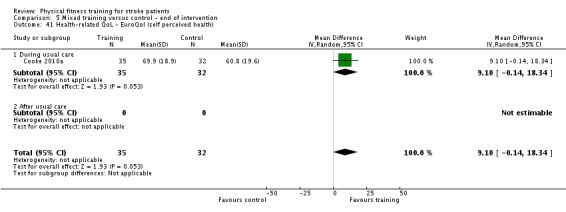
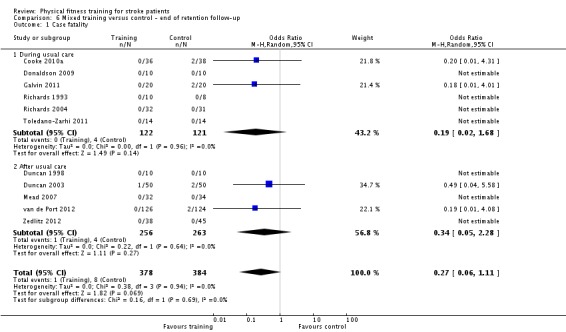
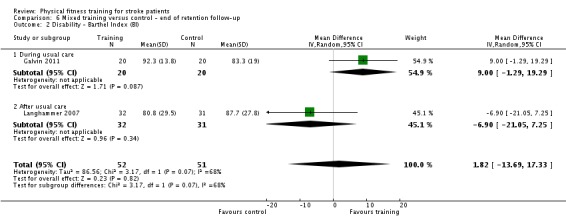
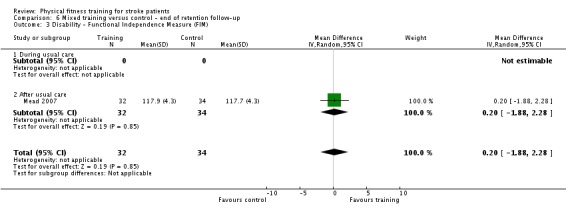
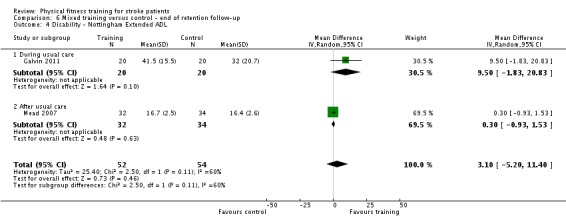
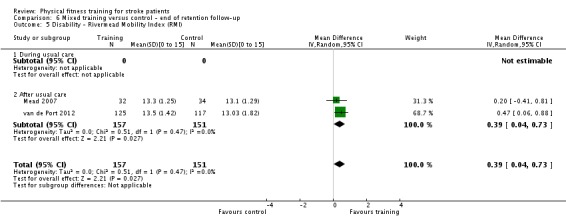
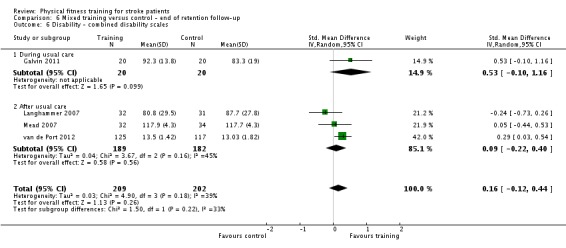
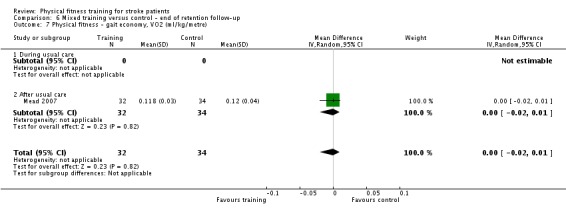
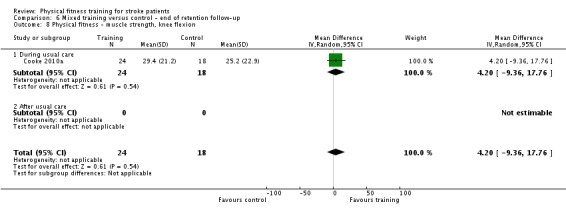
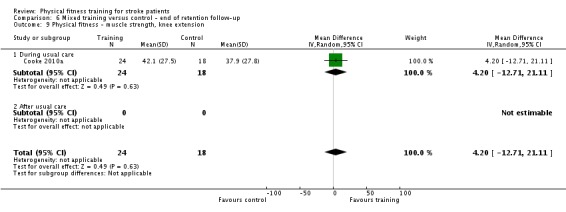
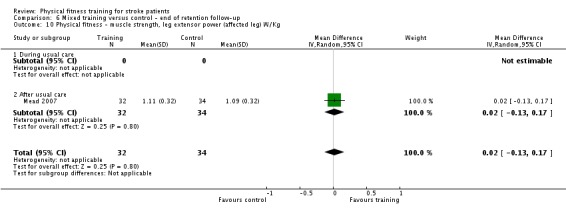
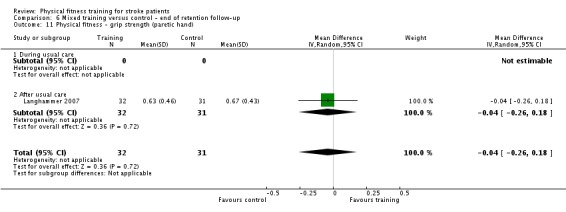
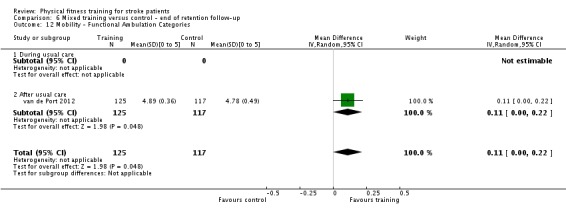
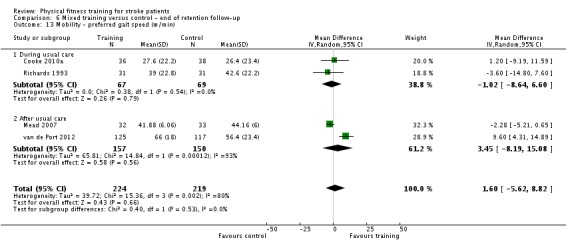
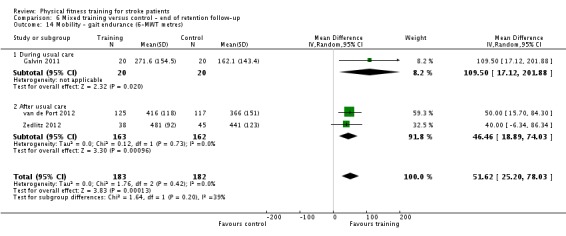
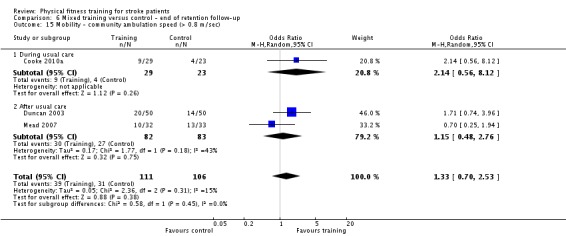
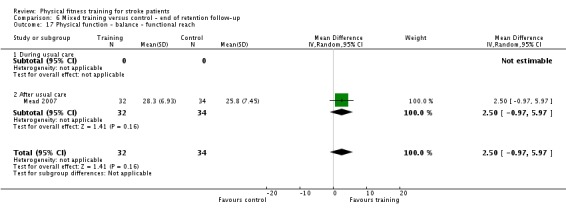
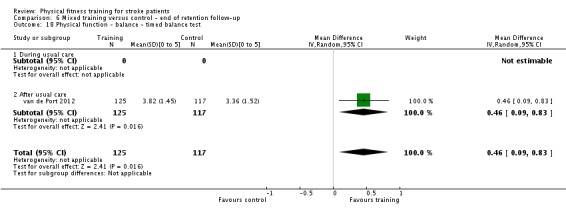
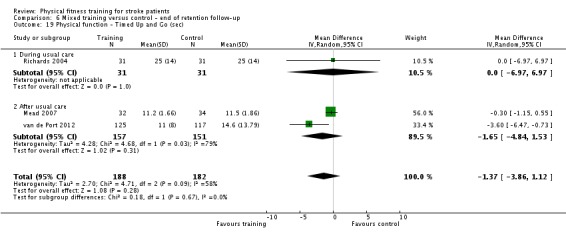
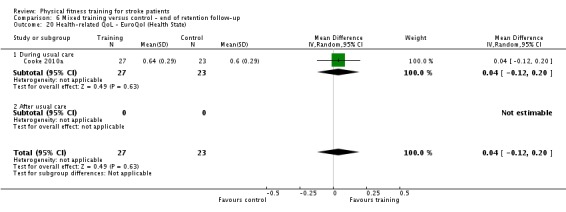
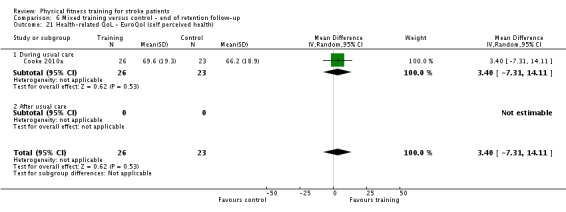
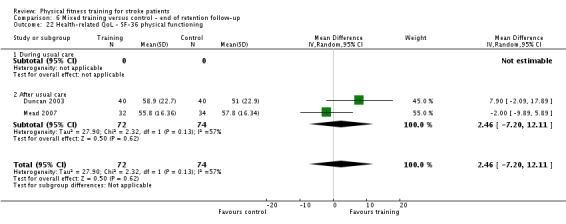
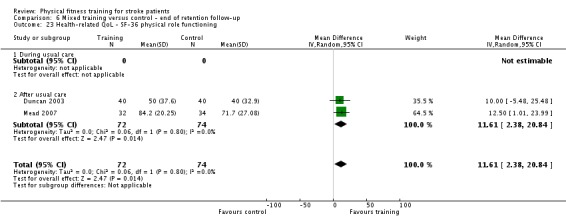
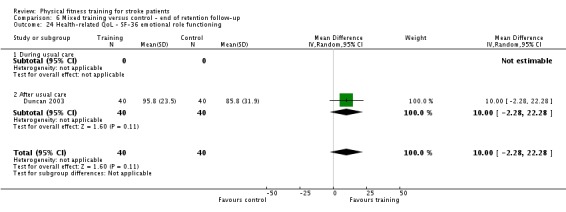
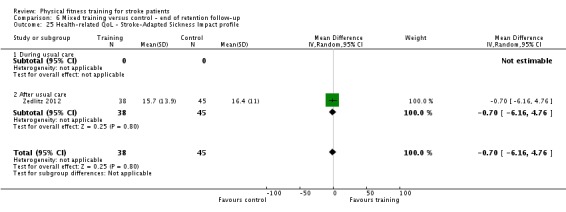
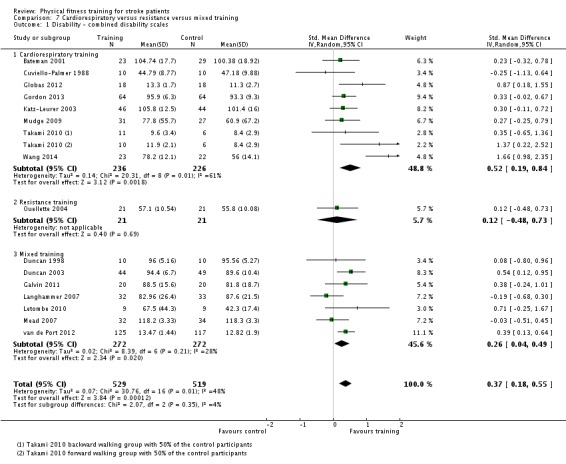
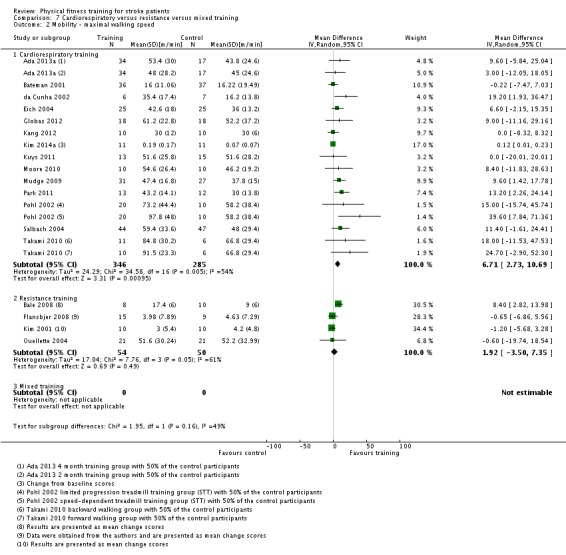
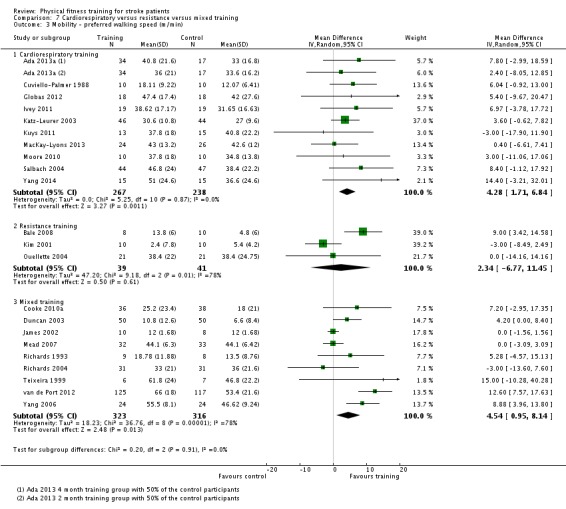
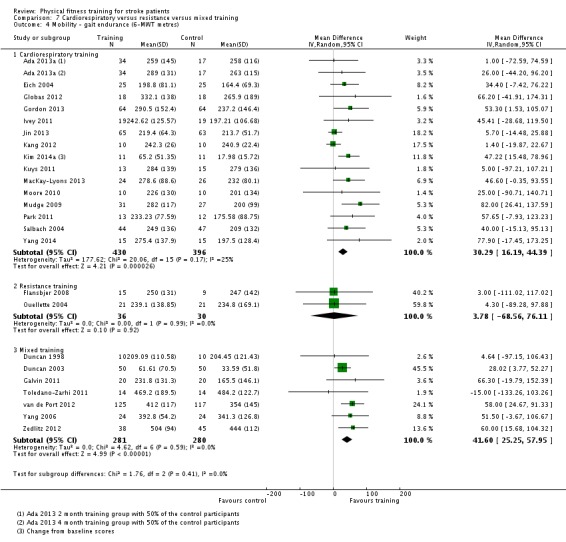
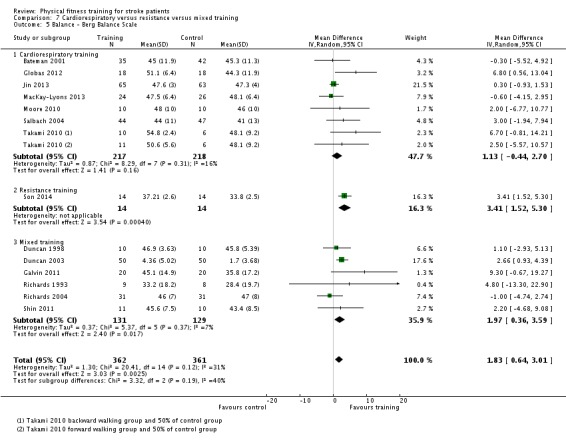
Main results: We included 58 trials, involving 2797 participants, which comprised cardiorespiratory interventions (28 trials, 1408 participants), resistance interventions (13 trials, 432 participants), and mixed training interventions (17 trials, 957 participants). Thirteen deaths occurred before the end of the intervention and a further nine before the end of follow-up. No dependence data were reported. Diverse outcome measures restricted pooling of data. Global indices of disability show moderate improvement after cardiorespiratory training (standardised mean difference (SMD) 0.52, 95% confidence interval (CI) 0.19 to 0.84; P value = 0.002) and by a small amount after mixed training (SMD 0.26, 95% CI 0.04 to 0.49; P value = 0.02); benefits at follow-up (i.e. after training had stopped) were unclear. There were too few data to assess the effects of resistance training.Cardiorespiratory training involving walking improved maximum walking speed (mean difference (MD) 6.71 metres per minute, 95% CI 2.73 to 10.69), preferred gait speed (MD 4.28 metres per minute, 95% CI 1.71 to 6.84), and walking capacity (MD 30.29 metres in six minutes, 95% CI 16.19 to 44.39) at the end of the intervention. Mixed training, involving walking, increased preferred walking speed (MD 4.54 metres per minute, 95% CI 0.95 to 8.14), and walking capacity (MD 41.60 metres per six minutes, 95% CI 25.25 to 57.95). Balance scores improved slightly after mixed training (SMD 0.27, 95% CI 0.07 to 0.47). Some mobility benefits also persisted at the end of follow-up. The variability, quality of the included trials, and lack of data prevents conclusions about other outcomes and limits generalisability of the observed results.
Authors' conclusions: Cardiorespiratory training and, to a lesser extent, mixed training reduce disability during or after usual stroke care; this could be mediated by improved mobility and balance. There is sufficient evidence to incorporate cardiorespiratory and mixed training, involving walking, within post-stroke rehabilitation programmes to improve the speed and tolerance of walking; some improvement in balance could also occur. There is insufficient evidence to support the use of resistance training. The effects of training on death and dependence after stroke are still unclear but these outcomes are rarely observed in physical fitness training trials. Cognitive function is under-investigated despite being a key outcome of interest for patients. Further well-designed randomised trials are needed to determine the optimal exercise prescription and identify long-term benefits.
Conflict of interest statement
DH Saunders and CA Greig were co‐authors of one included study (Mead 2007). GE Mead has received research funding for exercise after stroke. She has received honoraria from Later Life Training to develop an educational course of exercise after stroke for exercise professionals. She has also received honoraria and expenses to present work on exercise after stroke at conferences. She has led a trial of exercise after stroke that is included in the review (Mead 2007). S Hayes has no declarations of interest. M Brazzelli has no declarations of interest.
Figures


Update of
-
Physical fitness training for stroke patients.Cochrane Database Syst Rev. 2013 Oct 21;(10):CD003316. doi: 10.1002/14651858.CD003316.pub5. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2016 Mar 24;3:CD003316. doi: 10.1002/14651858.CD003316.pub6. PMID: 24142492 Updated.
References
References to studies included in this review
-
- Ada L, Dean CM, Lindley R. Randomized trial of treadmill training to improve walking in community‐dwelling people after stroke: the AMBULATE trial. International Journal of Stroke 2013;8(6):436‐44. - PubMed
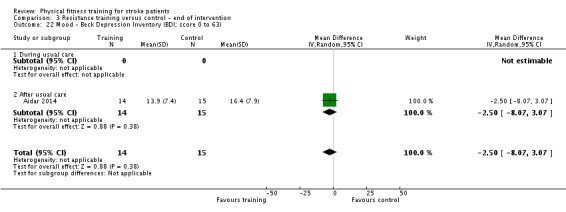
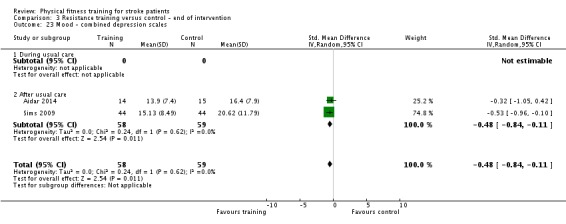
- Dean CM, Ada L, Lindley RI. Treadmill training provides greater benefit to the subgroup of community‐dwelling people after stroke who walk faster than 0.4m/s: a randomised trial. Journal of Physiotherapy (Australian Physiotherapy Association) 2014;60(2):97‐101. - PubMed
-
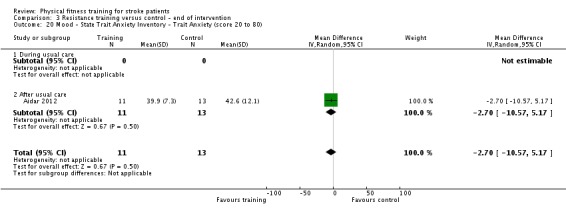
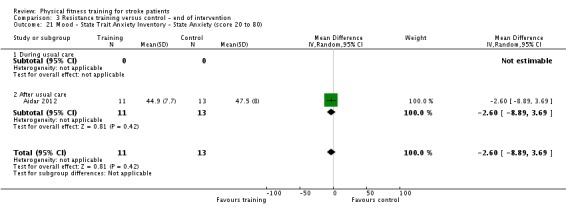
- Aidar FJ, Silva AJ, Reis VM, Carniero A, Carniero‐Cotta S. A study on the quality of life in ischaemic vascular accidents and its relation to physical activity [Estudio de la calidad de vida en el accidente vascular isquémico y su relación con la acividad física]. Revista de Neurología 2007;45:518‐22. - PubMed
-
- Bale M, Strand LI. Does functional strength training of the leg in subacute stroke improve physical performance? A pilot randomized controlled trial. Clinical Rehabilitation 2008;22(10‐11):911‐21. - PubMed
References to studies excluded from this review
-
- Ada L, Dean CM, Hall JM, Bampton J, Crompton S. A treadmill and overground walking program improves walking in individuals residing in the community after stroke: a placebo‐controlled randomised trial. Internal Medicine Journal 2004;34(1‐2):A7. - PubMed
- Ada L, Dean CM, Hall JM, Bampton J, Crompton S. A treadmill and overground walking program improves walking in persons residing in the community after stroke: a placebo‐controlled, randomized trial. Archives of Physical Medicine and Rehabilitation 2003;84(10):1486‐91. - PubMed
-
- Ada L, Dean CM, Morris ME, Simpson JM, Katrak P. Randomized trial of treadmill walking with body weight support to establish walking in subacute stroke. The MOBILISE Trial. Stroke 2010;41:1237‐42. - PubMed
-
- Adie K, Schofield C, Berrow M, Pritchard C, Freeman J, Humfryes J, et al. Does the use of Nintendo Wii Sports improve arm function and is it acceptable to patients after stroke? Publication of the protocol of the Trial of Wii in Stroke ‐ TWIST. International Journal of General Medicine 2014;7:475‐81. - PMC - PubMed
-
- Aidar F, Garrido N, Silva A, Reis V, Marinho D, Oliveira RJ. Effects of aquatic exercise on depression and anxiety in ischemic stroke subjects. Health 2013;5(2):222‐8.
-
- Akbari A, Karimi H. The effect of strengthening exercises on exaggerated muscle tonicity in chronic hemiparesis following stroke. Journal of Medical Sciences 2006;6(3):382‐8.
References to studies awaiting assessment
-
- Arya K, Verma R, Garg RK, Sharma VP, Agarwal M, Aggarwal GG. Meaningful Task‐Specific Training (MTST) for stroke rehabilitation: a randomized controlled trial. Topics in Stroke Rehabilitation 2012;19(3):193‐211. - PubMed
-
- Askim T, Morkved S, Engen A, Roos K, Aas T, Indredavik B. Effects of a community‐based intensive motor training program combined with early supported discharge after treatment in a comprehensive stroke unit: a randomized, controlled trial. Stroke 2010;41(8):1697‐703. - PubMed
-
- Buyukavci R, Iahin F, Sat S, Dotu B, Kuran B. The effect of trunk balance training on motor recovery, trunk balance, ambulation and quality of life in subacute stroke patients: a randomized controlled trial. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2011;57:270.
-
- Byun SD, Jung TD, Kim CH, Lee YS. Effects of the sliding rehabilitation machine on balance and gait in chronic stroke patients ‐ a controlled clinical trial. Clinical Rehabilitation 2011;25(5):408‐15. - PubMed
-
- Dean CM, Ada L, Bampton J, Morris ME, Katrak PH, Potts S. Treadmill walking with body weight support in subacute non‐ambulatory stroke improves walking capacity more than overground walking: a randomised trial. Journal of Physiotherapy 2010;56(2):97‐103. - PubMed
References to ongoing studies
-
- Brauer S. The efficacy of a novel, non‐robotic intervention to train reaching post stroke. ANZCTR. [ ACTRN12608000457347 ]
- Brauer S, Hayward K, Carson R, Cresswell A, Barker R. The efficacy of SMART Arm training early after stroke for stroke survivors with severe upper limb disability: a protocol for a randomised controlled trial. BMC Neurology 2013;13:71. - PMC - PubMed
-
- English C, Bernhardt J, Crotty M, Esterman A, Segal L, Hillier S. Circuit class therapy or seven‐day week therapy for increasing rehabilitation intensity of therapy after stroke (CIRCIT): a randomized controlled trial. International Journal of Stroke 2015;10(4):594‐602. - PubMed
- English C, Bernhardt J, Hillier S. Circuit class therapy and 7‐day‐week therapy increase physiotherapy time, but not patient activity: early results from the CIRCIT Trial. Stroke 2014;45(10):3002‐7. - PubMed
- Hillier S. Circuit class therapy for rehabilitation after stroke. A pragmatic randomised controlled trial (CIRCIT). ANZCTR. [ACTRN12610000096055]
- Hillier S, English C, Bernhardt J, Crotty M, Esterman A, Segal L. Free communications 3: Multidisciplinary rehabilitation circuit class and 7‐day week therapy for increasing rehabilitation intensity of therapy after stroke (CIRCIT): Six month follow‐up and cost analysis of the CIRCIT RCT. International Journal of Stroke 2014;9:21.
- Hillier S, English C, Crotty M, Segal L, Bernhardt J, Esterman A. Circuit class or seven‐day therapy for increasing intensity of rehabilitation after stroke: protocol of the CIRCIT trial. International Journal of Stroke 2011;6(6):560‐5. - PubMed
-
- Reynolds J. The effect of moderate‐intensity cardiovascular fitness training compared to standard care in people with a diagnosis of stroke: a pilot randomised controlled trial. ANZCTR. [ACTRN12613000822785]
-
- Hariohm K, Prakash V, Vasanthan R, Daran JKD, Samuel RJ. An RCT protocol on efficacy of deep knee flexion exercises on improving activities involving deep knee flexion and quality of life in persons with stroke. Cerebrovascular Diseases 2013;36:15.
-
- Pomeroy VM, Ward NS, Johansen‐Berg H, Vliet P, Burridge J, Hunter SM, et al. FAST INdiCATE Trial protocol. Clinical efficacy of functional strength training for upper limb motor recovery early after stroke: Neural correlates and prognostic indicators. International Journal of Stroke 2014;9(2):240‐5. - PMC - PubMed
- Walker A. Clinical efficacy of functional strength training for upper limb motor recovery early after stroke: neural correlates and prognostic indicators. http://www.controlled‐trials.com/ (accessed January 2013). - PMC - PubMed
Additional references
-
- American College of Sports Medicine. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Medicine and Science in Sports and Exercise 1998;30(6):975‐91. - PubMed
-
- Garber CE, Blissmer B, Deschenes MR, Franklin BA, LaMonte MJ, Lee IM, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine & Science in Sports & Exercise 2011;43(7):1334‐59. - PubMed
-
- Ada L, Dean CM, Nascimento LR, Teixeira‐Salmela LF. Treadmill training is effective for ambulatory adults with stroke: a systematic review. Journal of Physiotherapy 2013;59(2):73‐80. - PubMed
-
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry 1961;4:561‐71. - PubMed
-
- Bernhardt J, Dewey H, Thrift A, Donnan G. Inactive and alone: physical activity within the first 14 days of acute stroke unit care. Stroke 2004;35(4):1005‐9. - PubMed
References to other published versions of this review
-
- Brazzelli M, Saunders DH, Greig CA, Mead GE. Physical fitness training for stroke patients: a systematic review of the evidence. International Journal of Stroke2011; Vol. 6:11. - PubMed
-
- Brazzelli M, Saunders DH, Greig CA, Mead GE. Physical fitness training for patients with stroke updated review. Stroke 2012;43(4):E39‐40. - PubMed
-
- Saunders DH, Greig CA, Young A, Mead GE. Physical fitness training for acute stroke patients ‐ a systematic review. Cerebrovascular Diseases 2002;13 Suppl 3:63.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical