

Economic Analysis of Prostate-Specific Antigen Screening and Selective Treatment Strategies
- PMID: 27010943
- PMCID: PMC4945414
- DOI: 10.1001/jamaoncol.2015.6275
Economic Analysis of Prostate-Specific Antigen Screening and Selective Treatment Strategies
Abstract
Importance: Prostate-specific antigen (PSA) screening for prostate cancer is controversial. Experts have suggested more personalized or more conservative strategies to improve benefit-risk tradeoffs, but the value of these strategies-particularly when combined with increased conservative management for low-risk cases-is uncertain.
Objectives: To evaluate the potential cost-effectiveness of plausible PSA screening strategies and to assess the value added by increased use of conservative management among low-risk, screen-detected cases.
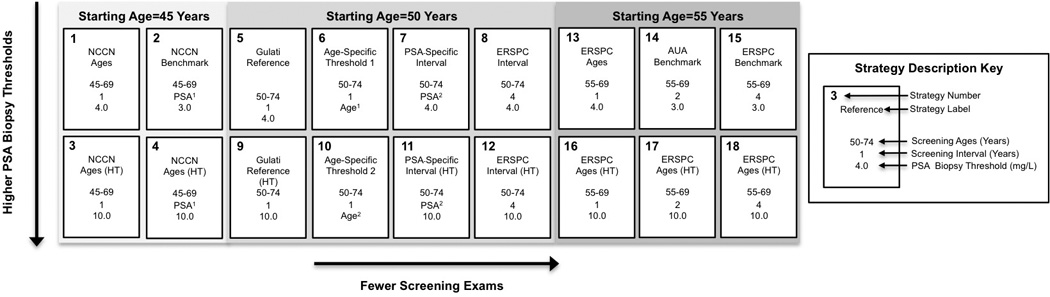
Design, setting, and participants: A microsimulation model of prostate cancer incidence and mortality was created. A simulated contemporary cohort of US men beginning at 40 years of age underwent 18 strategies for PSA screening. Treatment strategies included (1) contemporary treatment practices based on age and cancer stage and grade observed in the Surveillance, Epidemiology, and End Results program in 2010 or (2) selective treatment practices whereby cases with a Gleason score lower than 7 and clinical T2a stage cancer or lower are treated only after clinical progression, and all other cases undergo contemporary treatment practices. National and trial data on PSA growth, screening and biopsy patterns, incidence of prostate cancer, treatment distributions, treatment efficacy, mortality, health-related quality of life, and direct medical expenditure were analyzed. Data were collected from March 18, 2009, to August 15, 2014, and analyzed from November 20, 2012, to December 11, 2015.
Interventions: Eighteen screening strategies that vary by start and stop age, screening interval, and criteria for biopsy referral and contemporary or selective treatment practices.
Main outcomes and measures: Life-years (LYs), quality-adjusted life-years (QALYs), direct medical expenditure, and cost per LY and QALY gained.
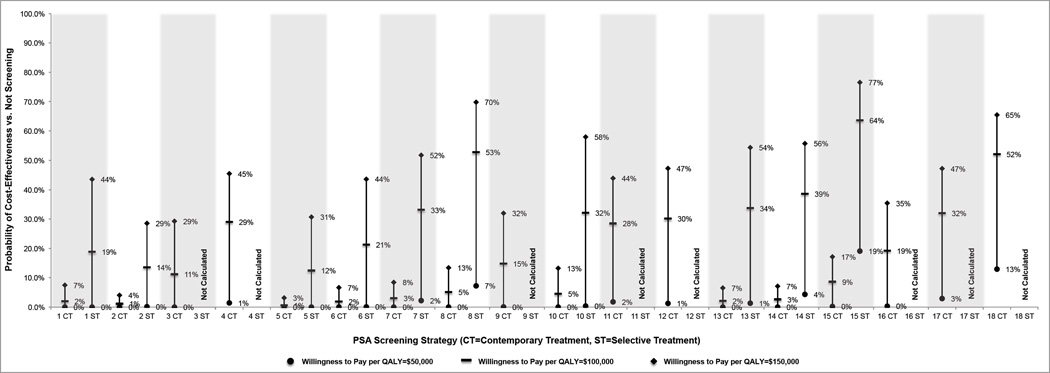
Results: All 18 screening strategies were associated with increased LYs (range, 0.03-0.06) and costs ($263-$1371) compared with no screening, with the cost ranging from $7335 to $21 649 per LY. With contemporary treatment, only strategies with biopsy referral for PSA levels higher than 10.0 ng/mL or age-dependent thresholds were associated with increased QALYs (0.002-0.004), and only quadrennial screening of patients aged 55 to 69 years was potentially cost-effective in terms of cost per QALY (incremental cost-effectiveness ratio, $92 446). With selective treatment, all strategies were associated with increased QALYs (0.002-0.004), and several strategies were potentially cost-effective in terms of cost per QALY (incremental cost-effectiveness ratio, $70 831-$136 332).
Conclusions and relevance: For PSA screening to be cost-effective, it needs to be used conservatively and ideally in combination with a conservative management approach for low-risk disease.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Does Prostate-Specific Antigen Screening Do More Good Than Harm?: Depends on How You Do It.JAMA Oncol. 2016 Jul 1;2(7):899-900. doi: 10.1001/jamaoncol.2015.6276. JAMA Oncol. 2016. PMID: 27010733 No abstract available.
-
Re: Economic Analysis of Prostate-Specific Antigen Screening and Selective Treatment Strategies.J Urol. 2016 Oct;196(4):1127-8. doi: 10.1016/j.juro.2016.07.057. Epub 2016 Jul 18. J Urol. 2016. PMID: 27628799 No abstract available.
References
-
- Moyer VA on behalf of the USPSTF. Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine. 2012;157(2):120–134. - PubMed
-
- Qaseem A, Barry MJ, Denberg TD, Owens DK, Shekelle P for the Clinical Guidelines Committee of the American College of P. Screening for Prostate Cancer: A Guidance Statement From the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2013 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
