

KRAS G12D Mutation Subtype Is A Prognostic Factor for Advanced Pancreatic Adenocarcinoma
- PMID: 27010960
- PMCID: PMC4822095
- DOI: 10.1038/ctg.2016.18
KRAS G12D Mutation Subtype Is A Prognostic Factor for Advanced Pancreatic Adenocarcinoma
Abstract
Objectives: There is no molecular biomarker available in the clinical practice to assess the prognosis of advanced pancreatic carcinoma. This multicenter prospective study aimed to investigate the role of KRAS mutation subtypes within the primary tumor to determine the prognosis of advanced pancreatic cancer.
Methods: The exon-2 KRAS mutation status was tested on endoscopic ultrasound-guided fine-needle aspiration biopsy material (primary tumor; restriction fragment-length polymorphism plus sequencing and TaqMan allelic discrimination) of patients with proven locally advanced and/or metastatic pancreatic ductal carcinoma. We used the Kaplan-Meier method, log-rank test, and Cox's model to evaluate the impact of KRAS status on the overall survival (OS), adjusting for age, stage of disease, clinical performance status, CA 19-9 levels, and treatment.
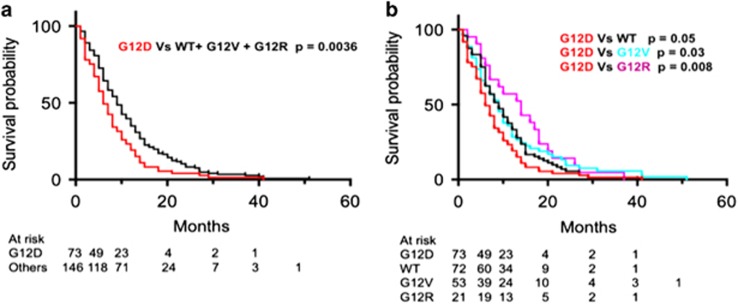
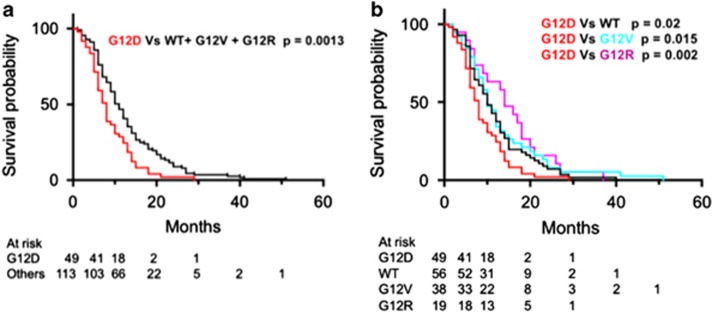
Results: A total of 219 patients (men: 116; mean age: 67±9.4 years) were included: 147 harbored a codon-12 KRAS mutation (G12D: 73; G12V: 53; G12R: 21) and 72 had a wild-type KRAS. There was no difference in the OS between patients with a mutant KRAS (8 months; 95% confidence interval (95% CI): 8.7-12.3) and the wild-type (9 months; 95% CI: 8.7-12.8; hazard ratio (HR): 1.03; P=0.82). However, the patients with a G12D mutation had a significantly shorter OS (6 months; 95% CI: 6.4-9.7) compared with the other patients (OS: 9 months; 95% CI: 10-13; HR: 1.47; P=0.003; i.e., wild type: 9 months, G12V: 9 months, G12R: 14 months). Similar results were observed in the subgroup of 162 patients who received chemotherapy (HR: 1.66; P=0.0013; G12D (n=49): 8 months, wild type (n=56): 10 months, G12V (n=38): 10 months, G12R (n=19): 14 months). Multivariate analyses identified KRAS G12D as an independent predictor for worse prognosis within the entire series (HR: 1.44; P=0.01) and in the subgroup of patients that received chemotherapy (HR: 1.84; P=0.02).
Conclusions: The KRAS G12D mutation subtype is an independent prognostic marker for advanced pancreatic ductal carcinoma. Codon and amino-acid-specific mutations of KRAS should be considered when evaluating the prognoses as well as in trials testing drugs that target RAS and downstream RAS pathways.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
