

Measurement of lateral acetabular coverage: a comparison between CT and plain radiography
- PMID: 27011864
- PMCID: PMC4732381
- DOI: 10.1093/jhps/hnv063
Measurement of lateral acetabular coverage: a comparison between CT and plain radiography
Abstract
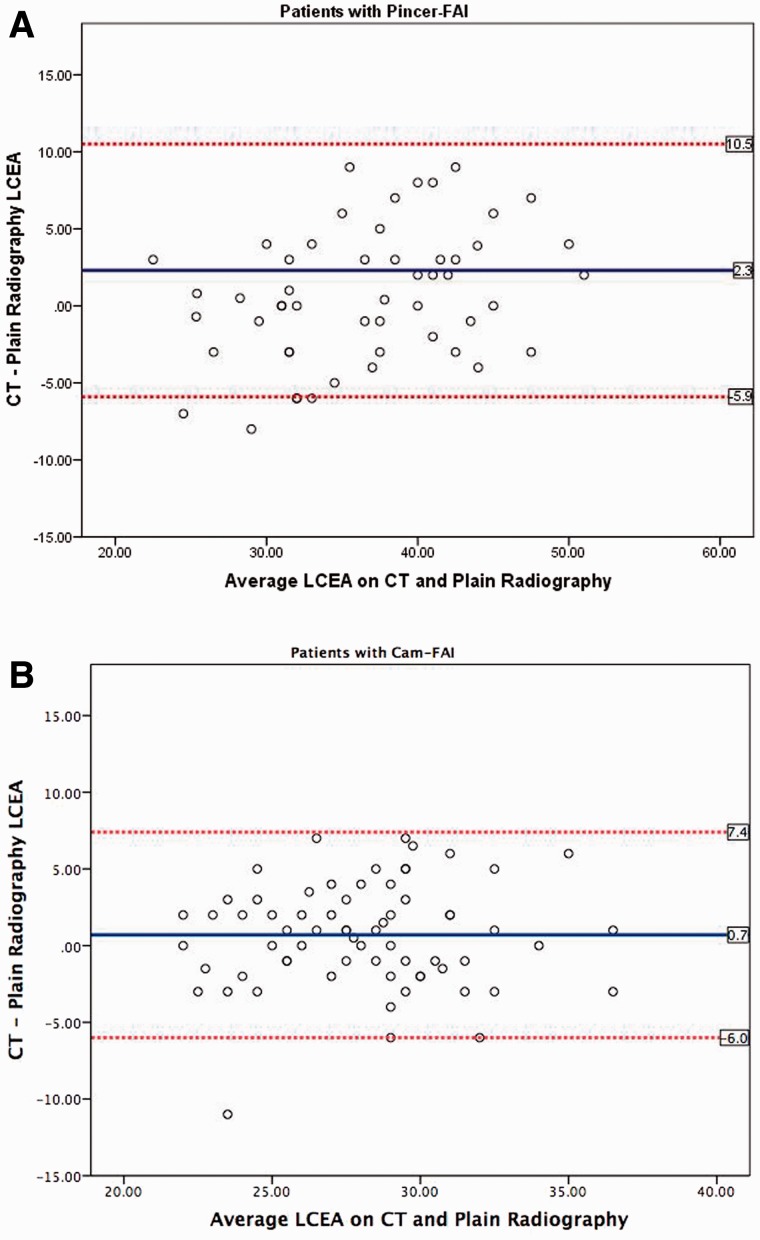
We prospectively evaluated the degree of absolute agreement between measurements of lateral center-edge angle (LCEA) on plain radiography (XR) and computed tomography (CT) in a consecutive cohort of 205 patients (410 hips) undergoing hip arthroscopy. Preoperative measurements of the LCEA were performed bilaterally utilizing standardized anteroposterior radiographs and coronal reformatted CT scans. Demographic variables including age, gender, height, weight, BMI and clinical diagnosis were recorded for all patients. Overall, measured values of the LCEA were 2.1° larger on CT compared with XR (32.9° versus 30.8°, P < 0.001). Subgroup analysis revealed the highest mean difference in hips with acetabular dysplasia and concomitant cam-type femoroacetabular impingement (FAI) [mean difference (CT-XR) 5.5°, 95% confidence interval (CI) 3.7°-7.3°, P = 0.011], followed by hips with isolated acetabular dysplasia (mean difference [CT-XR] 4.9°, 95% CI 2.7°-7.0°, P < 0.001). In contrast, 119 (29.0%) of the hips demonstrated larger measurements of the LCEA on 25 XR relative to CT. Of these hips, 20 (16.8%) had pincer-FAI and 25 had cam-FAI (21.0%), representing a significantly higher proportion compared with all other clinical subgroups (P = 0.045 and 0.036, respectively). Our study demonstrates measured values of the LCEA are consistently inflated on CT relative to XR for a wide variety of hip pathologies, highlighting the need for standardization and validation of CT-based measurements to improve the quality of clinical decision making.
Level of evidence: Diagnostic Level II.
Figures
References
-
- Wiberg G. Studies on dysplastic acetabulum and congenital subluxation of the hip joint with special reference to the complications of osteoarthritis. Acta Chir Scand 1939; 83(Suppl. 58): 1–135.
-
- Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis—what the radiologist should know. AJR Am J Roentgenol 2007; 188: 1540–52. - PubMed
-
- Jesse MK, Petersen B, Strickland C, et al. Normal anatomy and imaging of the hip: emphasis on impingement assessment. Semin Musculoskelet Radiol 2013; 17: 229–47. - PubMed
-
- Matsuda DK, Khatod M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy 2012; 28: 1738–43. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
