

Subtype-Specific Interactions and Prognosis in Cardiac Amyloidosis
- PMID: 27013539
- PMCID: PMC4943263
- DOI: 10.1161/JAHA.115.002877
Subtype-Specific Interactions and Prognosis in Cardiac Amyloidosis
Abstract
Background: Light chain (AL) and transthyretin (ATTR) amyloidosis have a similar effect on myocardial function but very different disease trajectories and survival. However, limited data are available evaluating subtype-specific predictors of outcomes in a large contemporary cohort.
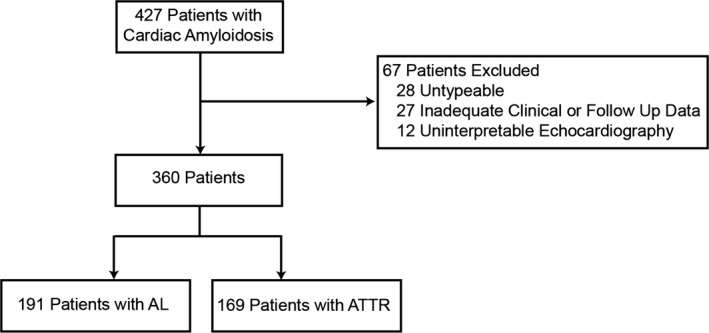
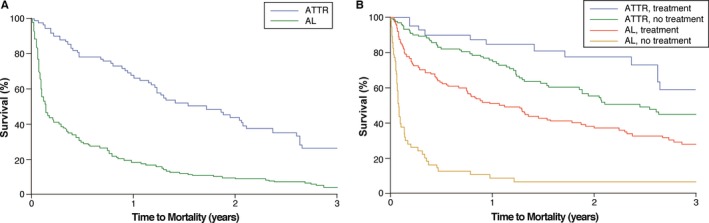
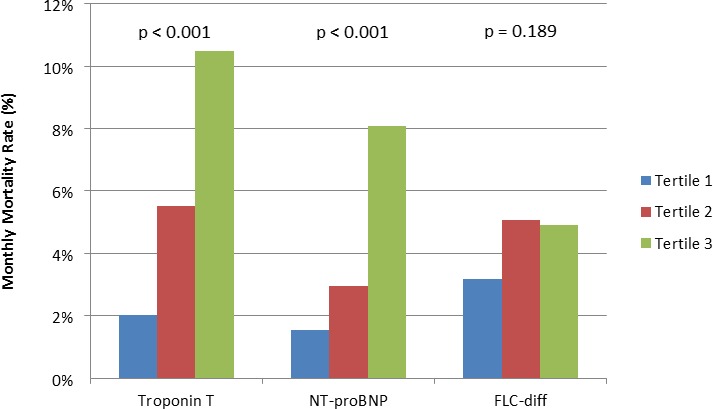
Methods and results: We retrospectively investigated 360 patients at the time of initial diagnosis of cardiac amyloidosis (191 AL and 169 ATTR) from 2002 to 2014. Clinical, laboratory, electrical, and morphologic covariates were evaluated based upon amyloid subtype. ATTR etiology was associated with older age, more chronic medical conditions, and the use of standard heart failure medical therapy. Left ventricular mass index and electrocardiographic voltage were higher in ATTR, while there was no difference in ejection fraction or markers of diastology between subtypes. A multivariable Cox model was generated using previously identified predictors of negative outcomes in cardiac amyloidosis and analyzed after stratification for subsequent amyloid-specific treatment. An AL etiology was the most predictive variable (hazard ratio 3.143, P<0.001) of 3-year all-cause mortality. The only covariate that showed a significantly greater magnitude of effect on mortality in 1 amyloid subtype versus the other was amyloid-specific treatment in AL (P=0.015). The magnitude of effect of other variables on mortality did not significantly differ between subtypes.
Conclusions: Clinical, morphological, electrical, and biomarker data do not significantly interact with amyloid subtype in its association with mortality, despite the fact that the prognosis in each subtype differs greatly. This suggests an additional factor or factors (such as light chain toxicity) contributing to poorer outcomes in AL amyloid.
Keywords: amyloid; cardiomyopathy; echocardiography; electrocardiography; prognosis.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Guidelines Working Group of UKMF, British Committee for Standards in Haematology BSfH . Guidelines on the diagnosis and management of AL amyloidosis. Br J Haematol. 2004;125:681–700. - PubMed
-
- Austin BA, Tang WH, Rodriguez ER, Tan C, Flamm SD, Taylor DO, Starling RC, Desai MY. Delayed hyper‐enhancement magnetic resonance imaging provides incremental diagnostic and prognostic utility in suspected cardiac amyloidosis. JACC Cardiovasc Imaging. 2009;2:1369–1377. - PubMed
-
- Phelan D, Collier P, Thavendiranathan P, Popovic ZB, Hanna M, Plana JC, Marwick TH, Thomas JD. Relative apical sparing of longitudinal strain using two‐dimensional speckle‐tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart. 2012;98:1442–1448. - PubMed
-
- Klein AL, Hatle LK, Taliercio CP, Oh JK, Kyle RA, Gertz MA, Bailey KR, Seward JB, Tajik AJ. Prognostic significance of Doppler measures of diastolic function in cardiac amyloidosis. A Doppler echocardiography study. Circulation. 1991;83:808–816. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
