

Heart Disease in Disorders of Muscle, Neuromuscular Transmission, and the Nerves
- PMID: 27014341
- PMCID: PMC4805555
- DOI: 10.4070/kcj.2016.46.2.117
Heart Disease in Disorders of Muscle, Neuromuscular Transmission, and the Nerves
Abstract
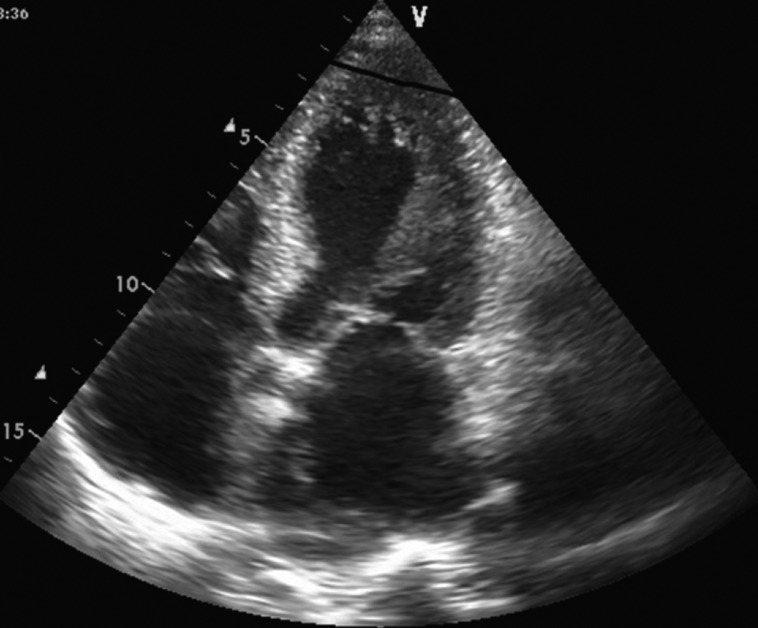
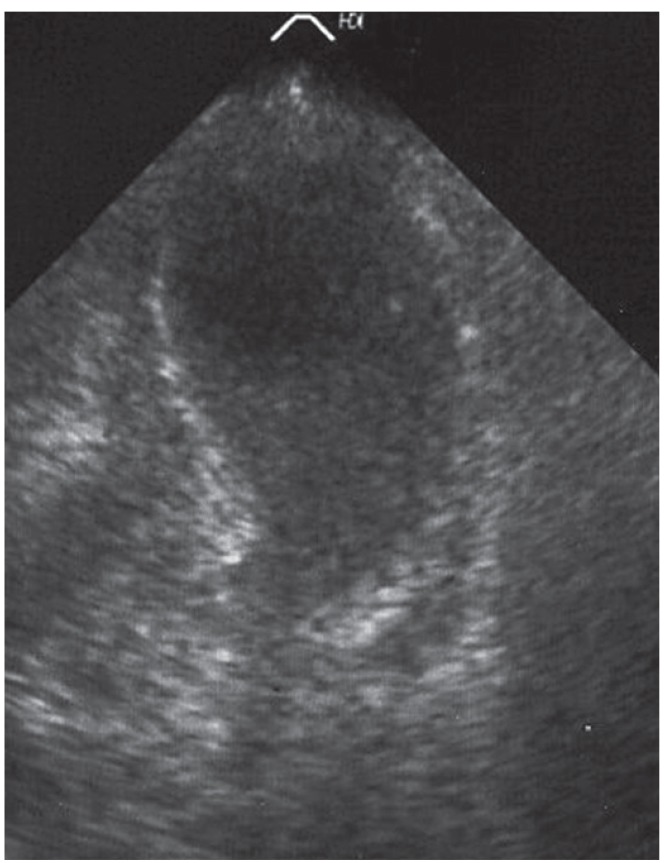
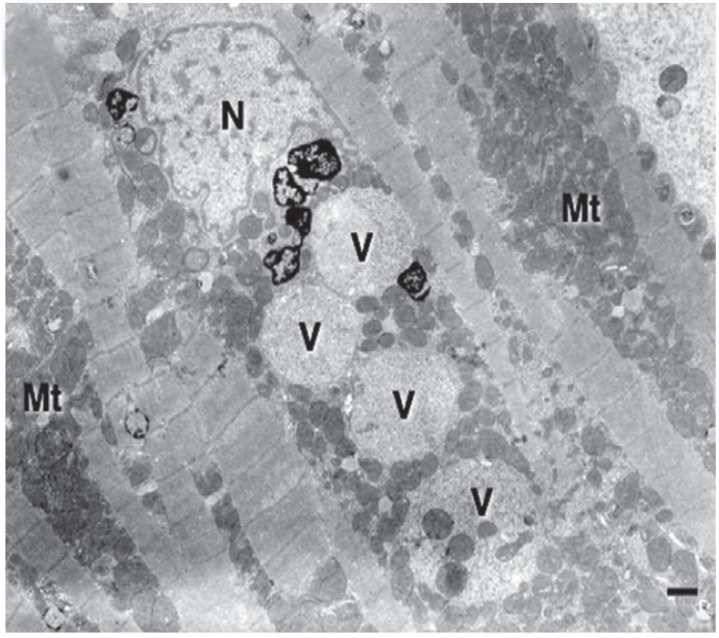
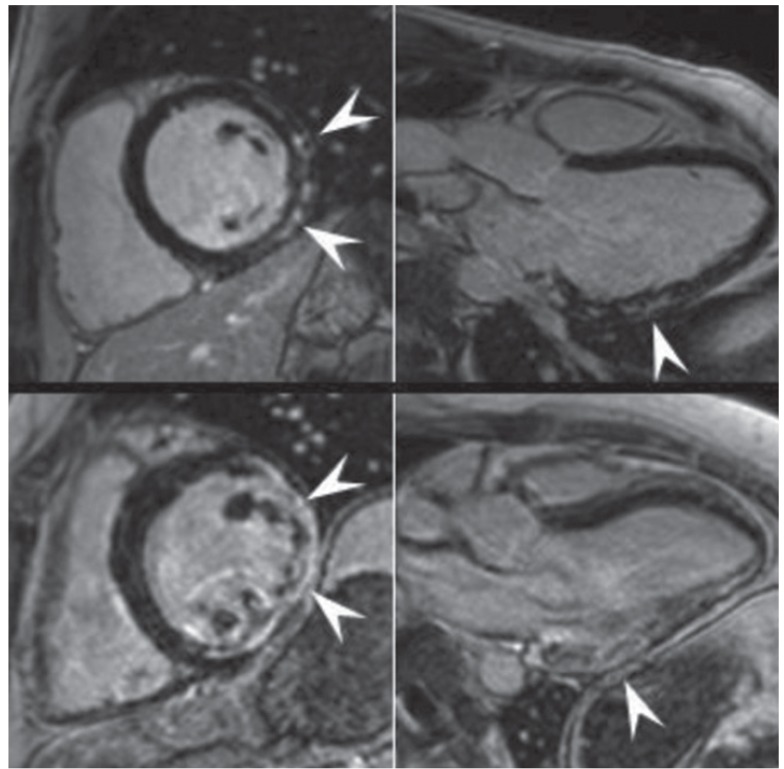
Little is known regarding cardiac involvement (CI) by neuromuscular disorders (NMDs). The purpose of this review is to summarise and discuss the major findings concerning the types, frequency, and severity of cardiac disorders in NMDs as well as their diagnosis, treatment, and overall outcome. CI in NMDs is characterized by pathologic involvement of the myocardium or cardiac conduction system. Less commonly, additional critical anatomic structures, such as the valves, coronary arteries, endocardium, pericardium, and even the aortic root may be involved. Involvement of the myocardium manifests most frequently as hypertrophic or dilated cardiomyopathy and less frequently as restrictive cardiomyopathy, non-compaction, arrhythmogenic right-ventricular dysplasia, or Takotsubo-syndrome. Cardiac conduction defects and supraventricular and ventricular arrhythmias are common cardiac manifestations of NMDs. Arrhythmias may evolve into life-threatening ventricular tachycardias, asystole, or even sudden cardiac death. CI is common and carries great prognostic significance on the outcome of dystrophinopathies, laminopathies, desminopathies, nemaline myopathy, myotonias, metabolic myopathies, Danon disease, and Barth-syndrome. The diagnosis and treatment of CI in NMDs follows established guidelines for the management of cardiac disease, but cardiotoxic medications should be avoided. CI in NMDs is relatively common and requires complete work-up following the establishment of a neurological diagnosis. Appropriate cardiac treatment significantly improves the overall long-term outcome of NMDs.
Keywords: Cardiac arrhythmias; Cardiomyopathies; Muscular diseases; Neuromuscular disease.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Rubin HJ, Lowbeer L. Progressive muscular dystrophy with involvement of heart muscle. Proc Staff Meet Tulsa Okla Hillcrest Meml Hosp. 1947;4:141–156. - PubMed
-
- Coelho E. Heart changes in the familial type of paramyloidosis with peripheral neuropathy. Z Kreislaufforsch. 1963;52:1066–1078. - PubMed
-
- Hertzman PA, Maddoux GL, Sternberg EM, et al. Repeated coronary artery spasm in a young woman with the eosinophilia-myalgia syndrome. JAMA. 1992;267:2932–2934. - PubMed
-
- Rakocević-Stojanović V, Pavlović S, Seferović P, et al. Pathohistological changes in endomyocardial biopsy specimens in patients with myotonic dystrophy. Panminerva Med. 1999;41:27–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
