

Predicting Left Ventricular Dysfunction after Surgery in Patients with Chronic Mitral Regurgitation: Assessment of Myocardial Deformation by 2-Dimensional Multilayer Speckle Tracking Echocardiography
- PMID: 27014352
- PMCID: PMC4805566
- DOI: 10.4070/kcj.2016.46.2.213
Predicting Left Ventricular Dysfunction after Surgery in Patients with Chronic Mitral Regurgitation: Assessment of Myocardial Deformation by 2-Dimensional Multilayer Speckle Tracking Echocardiography
Abstract
Background and objectives: The development of postoperative left ventricular (LV) dysfunction is a frequent complication in patients with chronic severe mitral valve regurgitation (MR) and portends a poor prognosis. Assessment of myocardial deformation enables myocardial contractility to be accurately estimated. The aim of the present study was to evaluate the predictive value of preoperative regional LV contractile function assessment using two-dimensional multilayer speckle-tracking echocardiography (2D MSTE) analysis in patients with chronic severe MR with preserved LV systolic function.
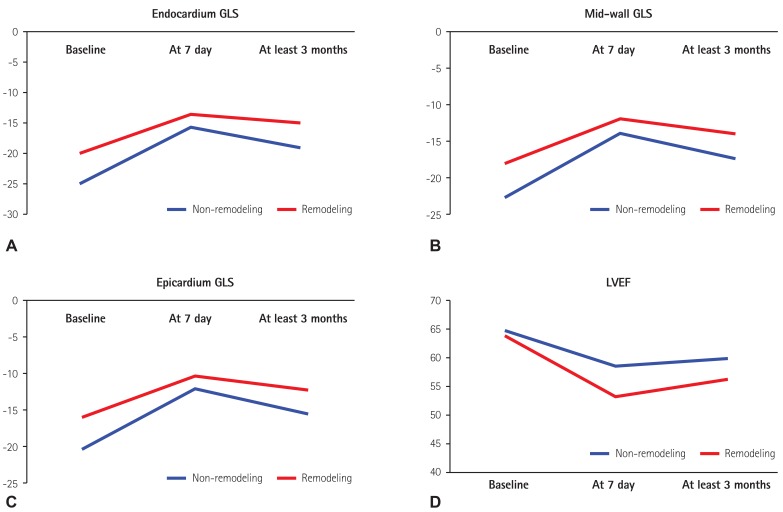
Subjects and methods: Forty-three consecutive patients with chronic severe MR with preserved LV systolic function scheduled for mitral valve replacement (MVR) or MV repair were prospectively enrolled. Serial echocardiographic studies were performed before surgery, at 7 days follow-up, and at least 3 months follow-up postoperatively. The conventional echocardiographic parameters were analyzed. Global longitudinal strain (GLS) was obtained quantitatively by 2D MSTE.
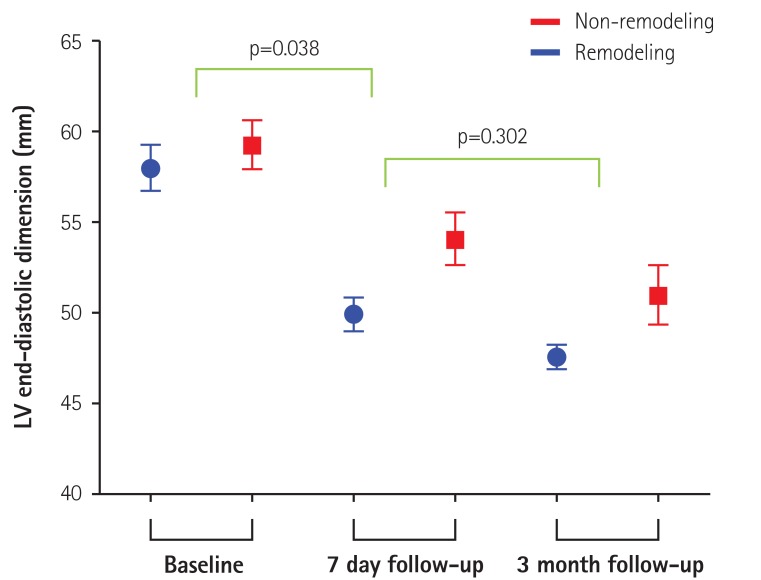
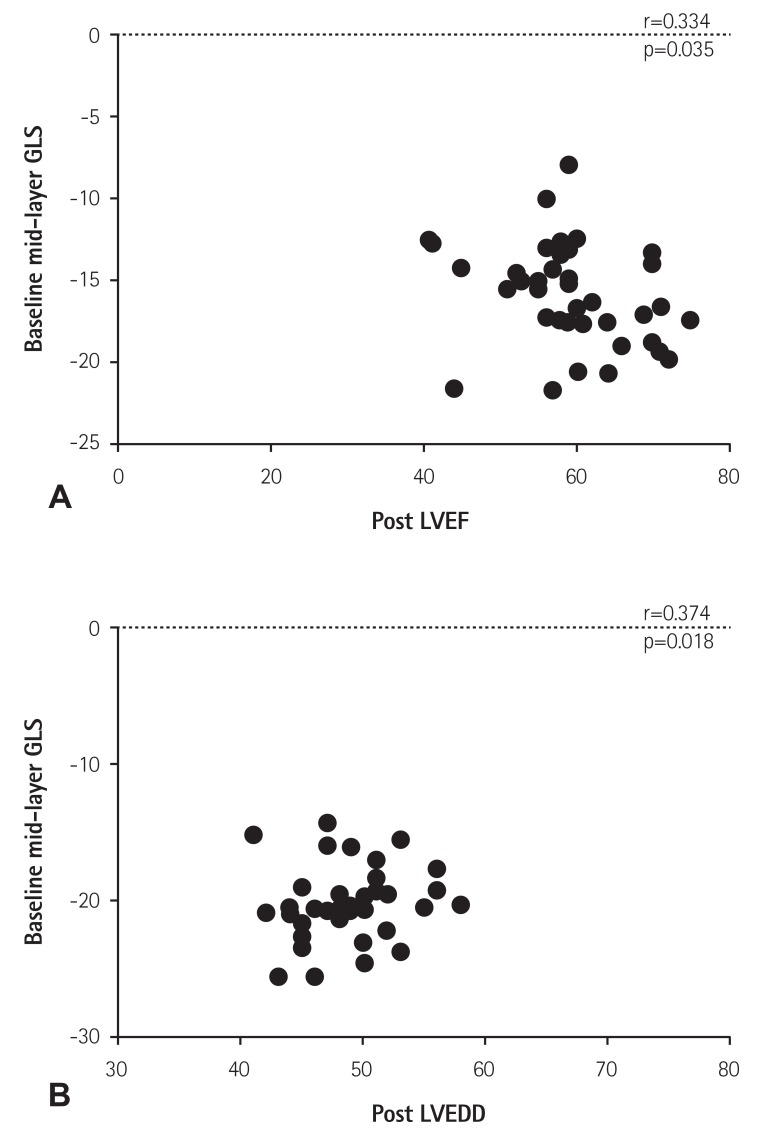
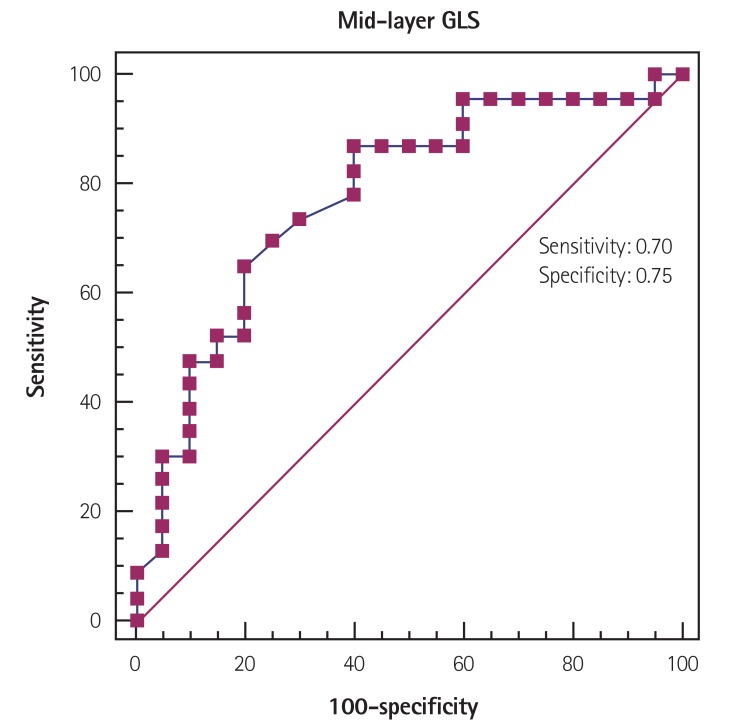
Results: The mean age of patients was 51.7±14.3 years and 25 (58.1%) were male. In receiver-operating characteristic curve analysis, the most useful cutoff value for discriminating postoperative LV remodeling in severe MR with normal LV systolic function was -20.5% of 2D mid-layer GLS. Patients were divided into two groups by the baseline GLS -20.5%. Preoperative GLS values strongly predicted postoperative LV remodeling or LV dysfunction. The postoperative degree of decrease in LV end-diastolic dimension might be an additive predictive factor.
Conclusion: STE can be used to predict a decrease in LV function after MVR in patients with chronic severe MR. This promising method could be of use in the clinic when trying to decide upon the optimum time to schedule surgery for such patients.
Keywords: Echocardiography; Mitral valve annuloplasty; Mitral valve annulus repair; Mitral valve insufficiency; Mitral valve regurgitation.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS) Vahanian A, et al. Guidelines on the management of valvular heart disease (version 2012) Eur Heart J. 2012;33:2451–2496. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2438–2488. - PubMed
-
- Witkowski TG, Thomas JD, Debonnaire PJ, et al. Global longitudinal strain predicts left ventricular dysfunction after mitral valve repair. Eur Heart J Cardiovasc Imaging. 2013;14:69–76. - PubMed
-
- Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, et al. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Engl J Med. 2005;352:875–883. - PubMed
-
- Rosenhek R, Rader F, Klaar U, et al. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation. 2006;113:2238–2244. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
