

Asthma Control Test and Bronchial Challenge with Exercise in Pediatric Asthma
- PMID: 27014666
- PMCID: PMC4782564
- DOI: 10.3389/fped.2016.00016
Asthma Control Test and Bronchial Challenge with Exercise in Pediatric Asthma
Abstract
Background: Poor asthma control can lead to exercise-induced bronchoconstriction (EIB), but the relationship between subjective disease control and EIB is unclear. No studies have compared asthma control test (ACT) scores of children with those of their parents regarding EIB. We assessed whether ACT scores predict the occurrence of EIB in two age groups. We also evaluated ACT scores and objective measures as explanatory variables for airway response to exercise.
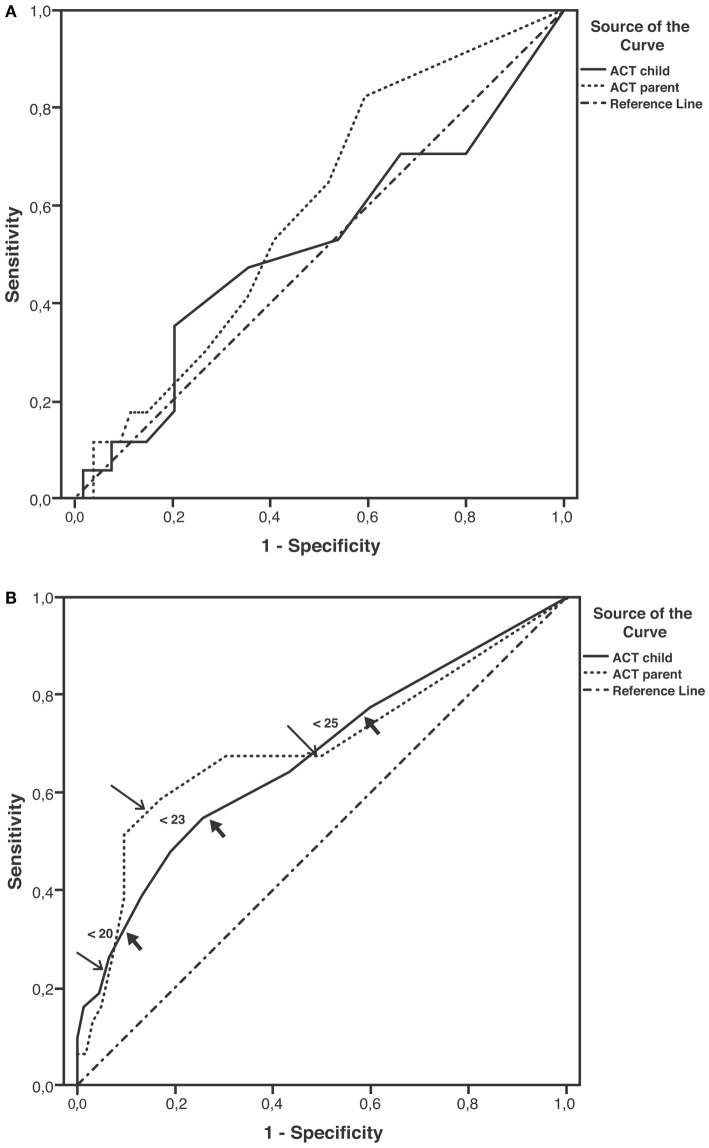
Methods: Patients (71, aged <12 years; 93, aged ≥12 years) and their parents completed an ACT questionnaire separately. Current therapy, skin prick testing, and spirometry at baseline and after exercise were assessed. EIB was defined as a fall in forced expiratory volume in 1 s (FEV1) of at least 12% from baseline. Sensitivity and specificity for cut-off values of ACT scores predictive of EIB were plotted, and the area under curve (AUC) was described.
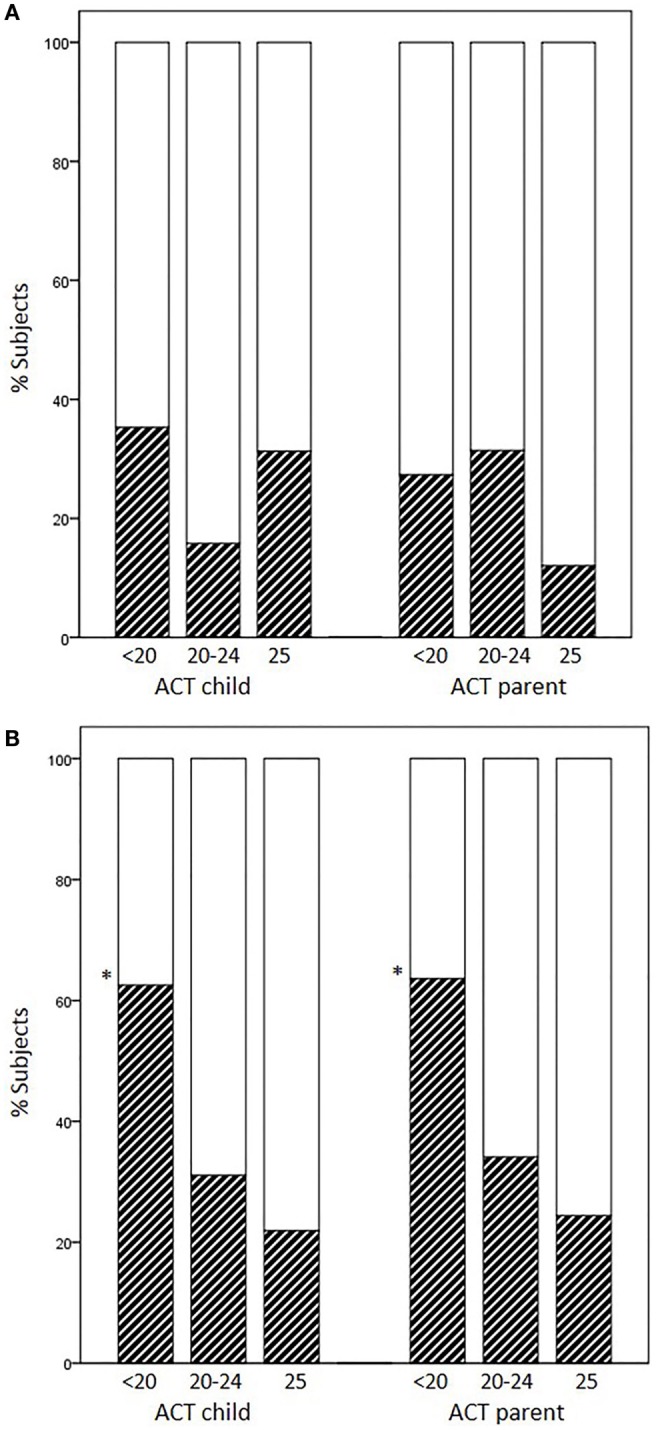
Results: Atopy and current therapy were similarly frequent. EIB was observed in 23.9% of children aged <12 years and in 33.3% of children aged ≥12 years. EIB occurrence in subjects previously scored as having full control (25), partial control (20-24), and no control (<20) varied according to the age group and responders. Percentages of EIB cases increased as ACT scores decreased in children aged ≥12 years alone (child ACT scores, 25: 21.9%, 20-24: 31.1%, <20: 62.5%, p = 0.017). Plots for ACT scores as predictors of EIB yielded low non-significant AUC values in children aged <12 years; in contrast, moderate AUC values emerged in children aged ≥12 years (child: 0.67, p = 0.007; parent: 0.69, p = 0.002). Sensitivity of ACT scores below 20 as a predictor of EIB was low in older children (child: 32.3%, parent: 22.6%), whereas specificity was high (child: 90.3%, parent: 93.5%). Multiple regression analysis with percent fall in FEV1 as dependent variable included FEV1/FVC%, ACT child score, and gender in the prediction model (r = 0.42, p = 0.000).
Conclusion: ACT scores are a more effective means of excluding than confirming EIB in asthmatic patients aged ≥12 years; their predictive value decreases in younger patients. ACT scores together with lung function may help to predict airway response to exercise. New tools for pediatric asthma assessment may optimize this association.
Keywords: asthma control test; atopy; children; exercise-induced bronchoconstriction; lung function; parents; questionnaires.
Figures
Similar articles
-
The Visual Analog Scale detects exercise-induced bronchoconstriction in children with asthma.J Asthma. 2020 Dec;57(12):1347-1353. doi: 10.1080/02770903.2019.1652640. Epub 2019 Sep 4. J Asthma. 2020. PMID: 31482747
-
Evaluation of association between exercise-induced bronchoconstriction and childhood asthma control test questionnaire scores in children.Pediatr Pulmonol. 2012 Mar;47(3):226-32. doi: 10.1002/ppul.21542. Epub 2011 Nov 4. Pediatr Pulmonol. 2012. PMID: 22058076
-
Cold air inhalation and exercise-induced bronchoconstriction in relationship to metacholine bronchial responsiveness: different patterns in asthmatic children and children with other chronic lung diseases.Respir Med. 1998 Feb;92(2):308-15. doi: 10.1016/s0954-6111(98)90114-7. Respir Med. 1998. PMID: 9616531 Clinical Trial.
-
Exhaled nitric oxide and other exhaled biomarkers in bronchial challenge with exercise in asthmatic children: current knowledge.Paediatr Respir Rev. 2015 Jan;16(1):68-74. doi: 10.1016/j.prrv.2013.11.006. Epub 2013 Nov 21. Paediatr Respir Rev. 2015. PMID: 24368252 Review.
-
Exercise-Induced Bronchospasm and Allergy.Front Pediatr. 2017 Jun 8;5:131. doi: 10.3389/fped.2017.00131. eCollection 2017. Front Pediatr. 2017. PMID: 28642859 Free PMC article. Review.
Cited by
-
Exercise-Induced Bronchoconstriction in Children: State of the Art from Diagnosis to Treatment.J Clin Med. 2024 Aug 5;13(15):4558. doi: 10.3390/jcm13154558. J Clin Med. 2024. PMID: 39124824 Free PMC article. Review.
-
Socio-demographic characteristics of children and young adults with varied asthma control- does it make a difference?Malawi Med J. 2022 Mar;34(1):31-36. doi: 10.4314/mmj.v34i1.6. Malawi Med J. 2022. PMID: 37265830 Free PMC article.
-
Difference in the Perceptions of Asthma Control Between Children With Asthma and Their Parents.Pediatr Pulmonol. 2025 Jan;60(1):e27457. doi: 10.1002/ppul.27457. Epub 2024 Dec 24. Pediatr Pulmonol. 2025. PMID: 39718118 Free PMC article.
-
Exercise-induced bronchoconstriction in children: Delphi study and consensus document about definition and epidemiology, diagnostic work-up, treatment, and follow-up.Respir Res. 2024 Dec 27;25(1):445. doi: 10.1186/s12931-024-03078-5. Respir Res. 2024. PMID: 39731113 Free PMC article.
-
Exercise-induced bronchoconstriction: prevalence, pathophysiology, patient impact, diagnosis and management.NPJ Prim Care Respir Med. 2018 Aug 14;28(1):31. doi: 10.1038/s41533-018-0098-2. NPJ Prim Care Respir Med. 2018. PMID: 30108224 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources