

Functional Results after Repair of Large Hiatal Hernia by Use of a Biologic Mesh
- PMID: 27014698
- PMCID: PMC4783575
- DOI: 10.3389/fsurg.2016.00016
Functional Results after Repair of Large Hiatal Hernia by Use of a Biologic Mesh
Abstract
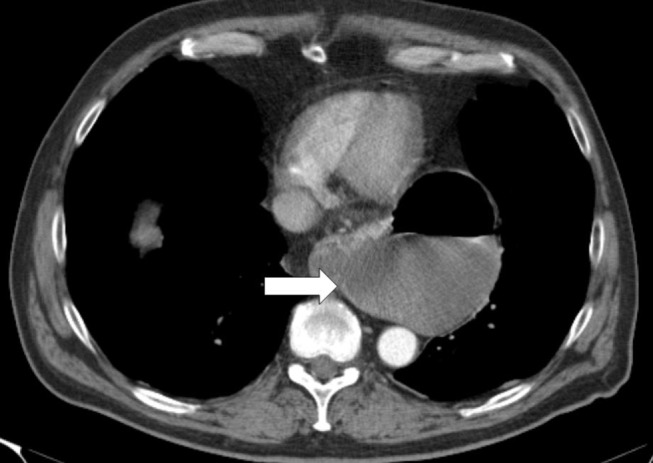
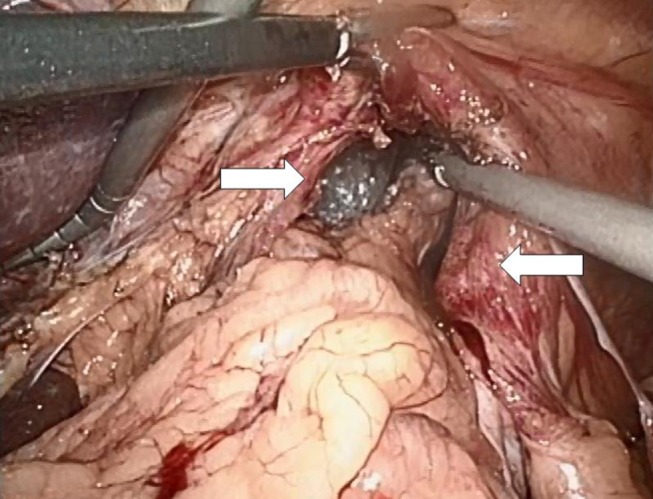
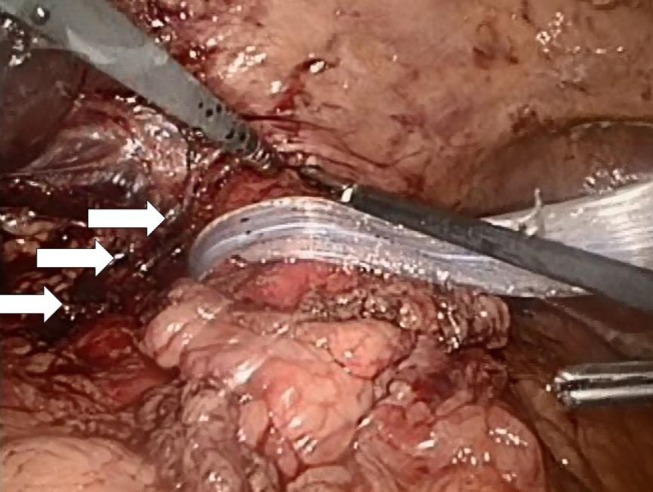
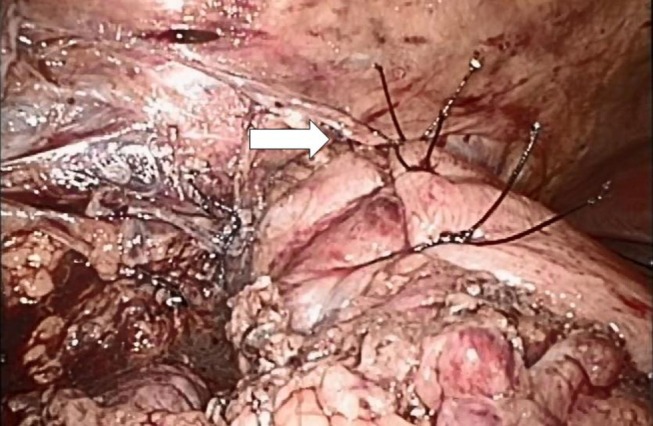
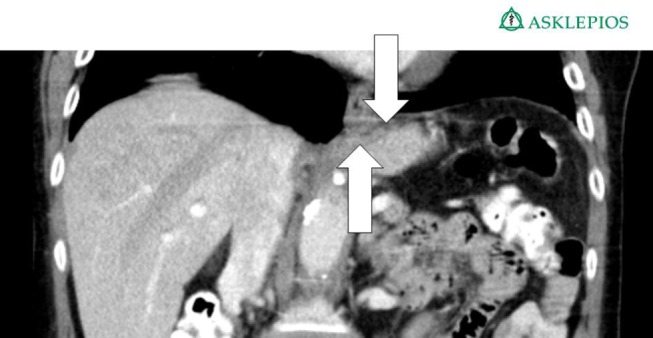
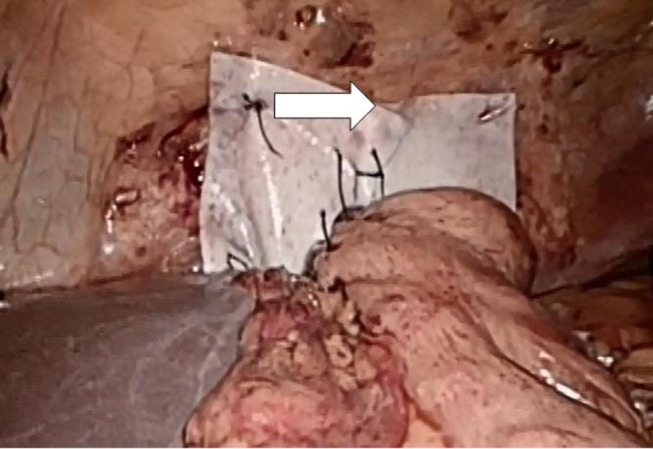
Background: The aim of this observational study is to analyze the results of patients with large hiatal hernia and upside-down stomach after surgical closure with a biological mesh (Permacol(®), Covidien, Neustadt an der Donau, Germany). Biological mesh is used to prevent long-term detrimental effects of artificial meshes and to reduce recurrence rates.
Methods: A total of 13 patients with a large hiatal hernia and endothoracic stomach, who underwent surgery between 2010 and 2014, were included. Interviews and upper endoscopy were conducted to determine recurrences, lifestyle restrictions, and current complaints.
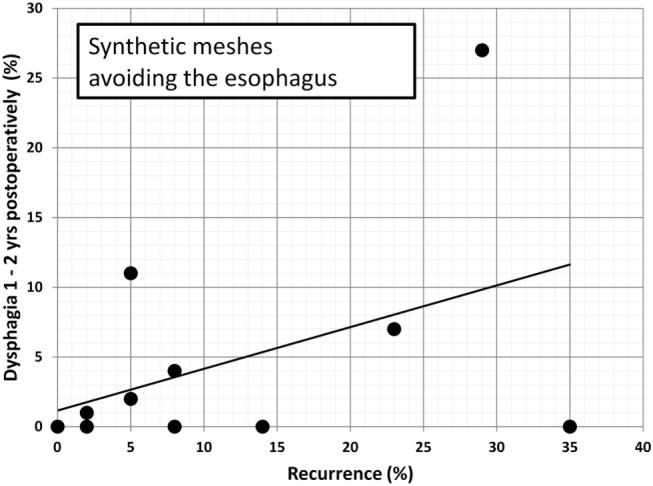
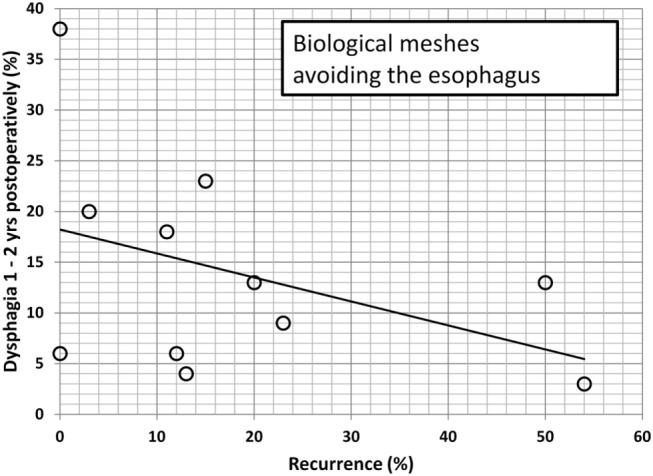
Results: After a mean follow-up of 26 ± 18 months (range: 3-58 months), 10 patients (3 men, mean age 73 ± 13, range: 26-81 years) were evaluated. A small recurrent axial hernia was found in one patient postoperatively. Dysphagia was the most common complaint (four cases); while in one case, the problem was solved after endoscopic dilatation. In three cases, bloat and postprandial pain were documented. In one case, an explantation of the mesh was necessary due to mesh migration and painful adhesions. In one further case with gastroparesis, pyloroplasty was performed without success. The data are compared to the available literature. It was found that dysphagia and recurrence rates are unrelated both in biological and in synthetic meshes if the esophagus is encircled. In series preserving the esophagus at least partially uncoated, recurrences after the use of biological meshes relieve dysphagia. After the application of synthetic meshes, dysphagia is aggravated by recurrences.
Conclusion: Recurrence is rare after encircling hiatal hernia repair with the biological mesh Permacol(®). Dysphagia, gas bloat, and intra-abdominal pain are frequent complaints. Despite the small number of patients, it can be concluded that a biological mesh may be an alternative to synthetic meshes to reduce recurrences at least for up to 2 years. Our study demonstrates that local fibrosis and thickening of the mesh can affect the outcome being associated with abdominal discomfort despite a successful repair. The review of the literature indicates comparable results after 2 years with both biologic and synthetic meshes embracing the esophagus. At the same point in time, reconstruction with synthetic and biologic materials differs when the esophagus is not or only partially encircled in the repair. This is important since encircling artificial meshes can erode the esophagus after 5-10 years.
Keywords: biologic mesh; complications; dysphagia; hiatal hernia repair; recurrence.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources