

New pattern-based personalized risk stratification system for endocervical adenocarcinoma with important clinical implications and surgical outcome
- PMID: 27016227
- PMCID: PMC5068220
- DOI: 10.1016/j.ygyno.2016.02.028
New pattern-based personalized risk stratification system for endocervical adenocarcinoma with important clinical implications and surgical outcome
Abstract
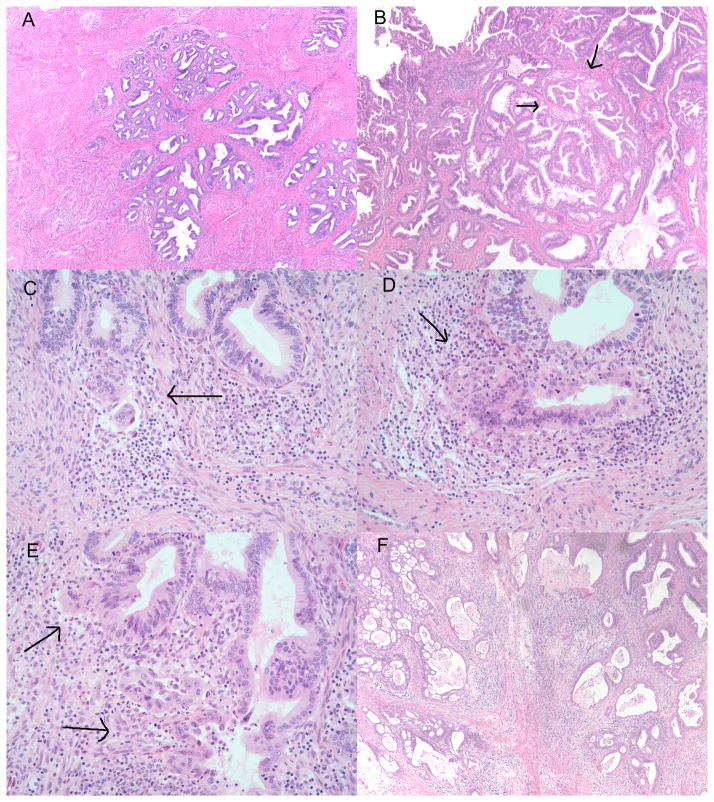
We present a recently introduced three tier pattern-based histopathologic system to stratify endocervical adenocarcinoma (EAC) that better correlates with lymph node (LN) metastases than FIGO staging alone, and has the advantage of safely predicting node-negative disease in a large proportion of EAC patients. The system consists of stratifying EAC into one of three patterns: pattern A tumors characterized by well-demarcated glands frequently forming clusters or groups with relative lobular architecture and lacking destructive stromal invasion or lymphovascular invasion (LVI), pattern B tumors demonstrating localized destructive invasion (small clusters or individual tumor cells within desmoplastic stroma often arising from pattern A glands), and pattern C tumors with diffusely infiltrative glands and associated desmoplastic response. Three hundred and fifty-two cases were included; mean follow-up 52.8 months. Seventy-three patients (21%) had pattern A tumors; all were stage I and there were no LN metastases or recurrences. Pattern B was seen in 90 tumors (26%); all were stage I and LVI was seen in 24 cases (26.6%). Nodal disease was found in only 4 (4.4%) pattern B tumors (one IA2, two IB1, one IB not further specified (NOS)), each of which showed LVI. Pattern C was found in 189 cases (54%), 117 had LVI (61.9%) and 17% were stage II or greater. Forty-five (23.8%) patients showed LN metastases (one IA1, 14 IB1, 5 IB2, 5 IB NOS, 11 II, 5 III and 4 IV) and recurrences were recorded in 41 (21.7%) patients. This new risk stratification system identifies a subset of stage I patients with essentially no risk of nodal disease, suggesting that patients with pattern A tumors can be spared lymphadenectomy. Patients with pattern B tumors rarely present with LN metastases, and sentinel LN examination could potentially identify these patients. Surgical treatment with nodal resection is justified in patients with pattern C tumors.
Keywords: Classification system; Endocervical adenocarcinoma; Invasive carcinoma; Lymph node metastasis; Pattern-based; Risk stratification.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that there are no conflicts of interest or funding to disclose.
Figures
References
-
- Diaz De Vivar A, Roma AA, Park KJ, Alvarado-Cabrero I, Rasty G, Chanona-Vilchis JG, et al. Invasive endocervical adenocarcinoma: proposal for a new pattern-based classification system with significant clinical implications: a multi-institutional study. Int J Gynecol Pathol. 2013;32:592–601. - PubMed
-
- Roma AA, Diaz De Vivar A, Park KJ, Alvarado-Cabrero I, Rasty G, Chanona-Vilchis JG, et al. Invasive Endocervical Adenocarcinoma: A New Pattern-based Classification System With Important Clinical Significance. Am J Surg Pathol. 2015;39:667–72. - PubMed
-
- Paquette C, Jeffus SK, Quick CM, Conaway MR, Stoler MH, Atkins KA. Interobserver variability in the application of a proposed histologic subclassification of endocervical adenocarcinoma. Am J Surg Pathol. 2015;39:93–100. - PubMed
-
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103–104. - PubMed
-
- Gien LT, Beauchemin MC, Thomas G. Adenocarcinoma: a unique cervical cancer. Gynecol Oncol. 2010;116:140–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
