

Review of Acute Traumatic Closed Mallet Finger Injuries in Adults
- PMID: 27019806
- PMCID: PMC4807168
- DOI: 10.5999/aps.2016.43.2.134
Review of Acute Traumatic Closed Mallet Finger Injuries in Adults
Abstract
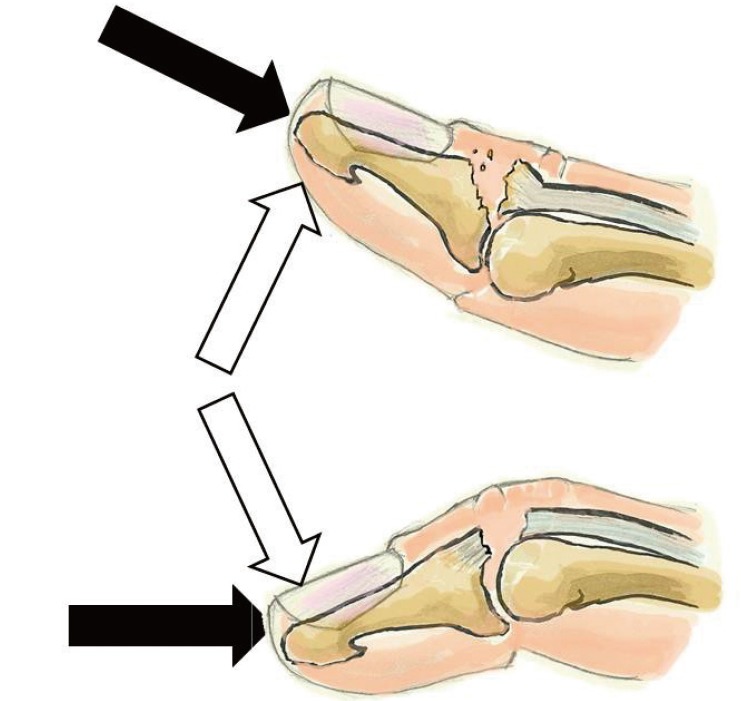
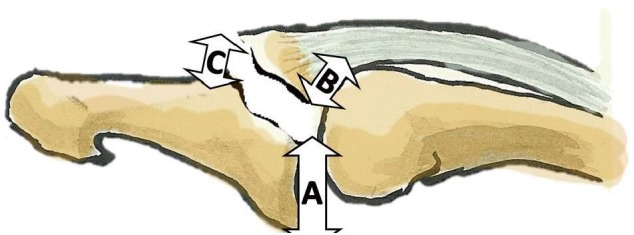
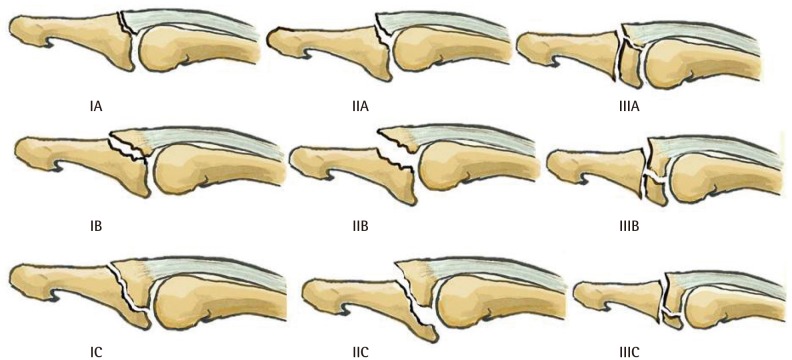
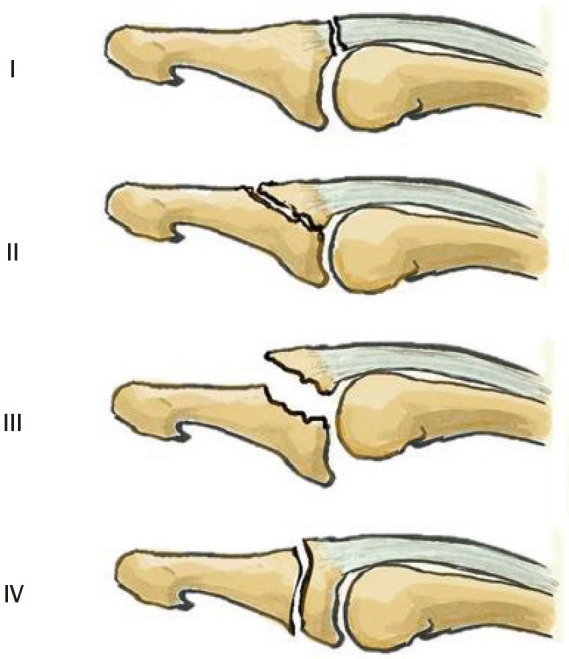
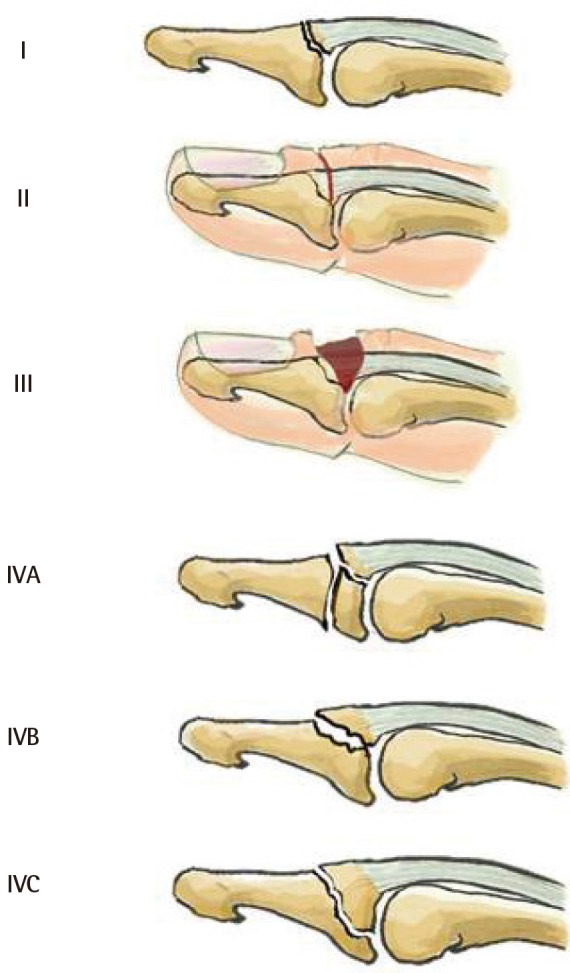
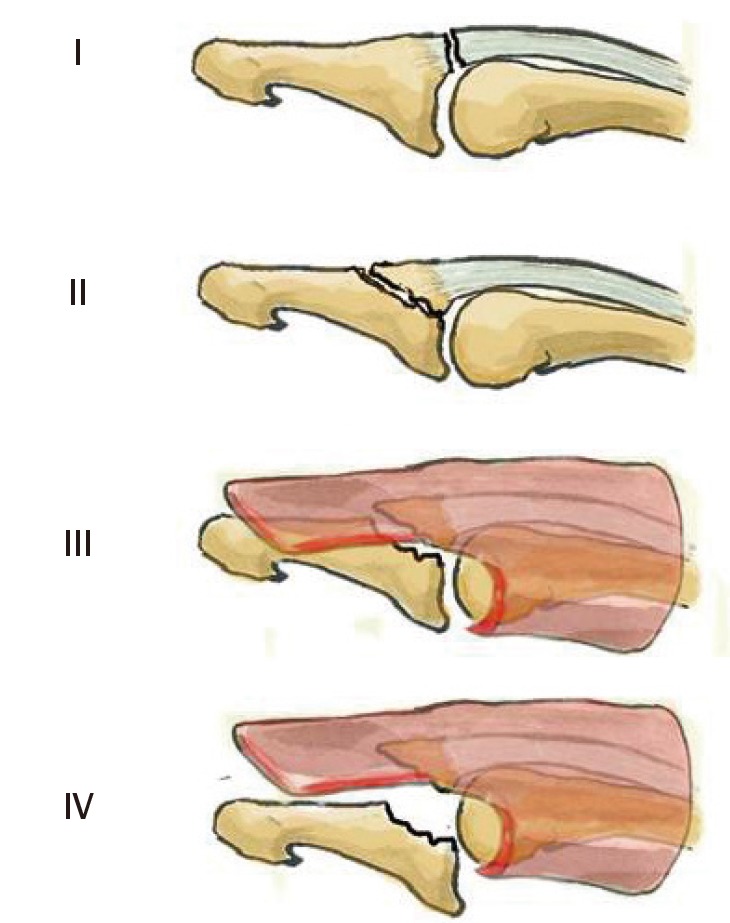
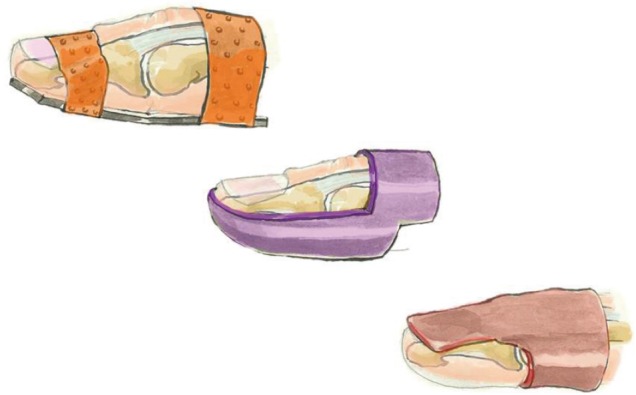
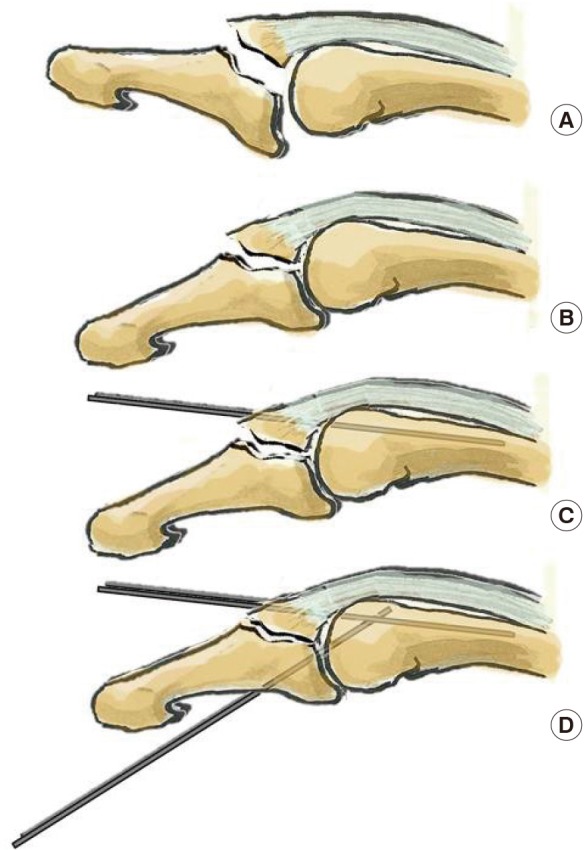
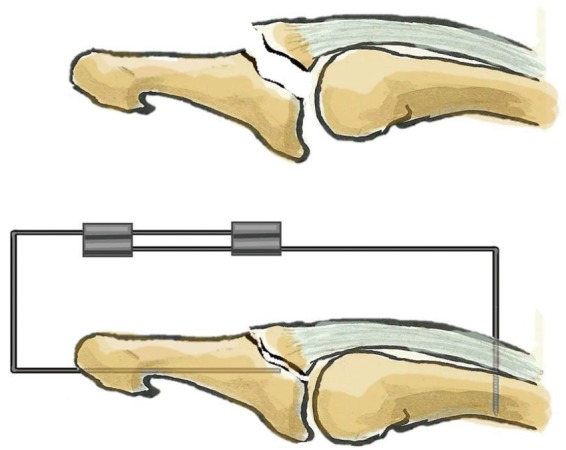
In adults, mallet finger is a traumatic zone I lesion of the extensor tendon with either tendon rupture or bony avulsion at the base of the distal phalanx. High-energy mechanisms of injury generally occur in young men, whereas lower energy mechanisms are observed in elderly women. The mechanism of injury is an axial load applied to a straight digit tip, which is then followed by passive extreme distal interphalangeal joint (DIPJ) hyperextension or hyperflexion. Mallet finger is diagnosed clinically, but an X-ray should always be performed. Tubiana's classification takes into account the size of the bony articular fragment and DIPJ subluxation. We propose to stage subluxated fractures as stage III if the subluxation is reducible with a splint and as stage IV if not. Left untreated, mallet finger becomes chronic and leads to a swan-neck deformity and DIPJ osteoarthritis. The goal of treatment is to restore active DIPJ extension. The results of a six- to eight-week conservative course of treatment with a DIPJ splint in slight hyperextension for tendon lesions or straight for bony avulsions depends on patient compliance. Surgical treatments vary in terms of the approach, the reduction technique, and the means of fixation. The risks involved are stiffness, septic arthritis, and osteoarthritis. Given the lack of consensus regarding indications for treatment, we propose to treat all cases of mallet finger with a dorsal glued splint except for stage IV mallet finger, which we treat with extra-articular pinning.
Keywords: Bony mallet; Mallet finger; Mallet fracture.
Conflict of interest statement
Philippe Liverneaux has conflict of interest with Newclip Technics and Argomedical. None of the other authors has conflit of interest.
Figures
References
-
- Badia A, Riano F. A simple fixation method for unstable bony mallet finger. J Hand Surg Am. 2004;29:1051–1055. - PubMed
-
- Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005;13:336–344. - PubMed
-
- Kronlage SC, Faust D. Open reduction and screw fixation of mallet fractures. J Hand Surg Br. 2004;29:135–138. - PubMed
-
- Abouna JM, Brown H. The treatment of mallet finger: the results in a series of 148 consecutive cases and a review of the literature. Br J Surg. 1968;55:653–667. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical