

A Modified, Direct Neck Lift Technique: The Cervical Wave-Plasty
- PMID: 27019811
- PMCID: PMC4807173
- DOI: 10.5999/aps.2016.43.2.181
A Modified, Direct Neck Lift Technique: The Cervical Wave-Plasty
Abstract
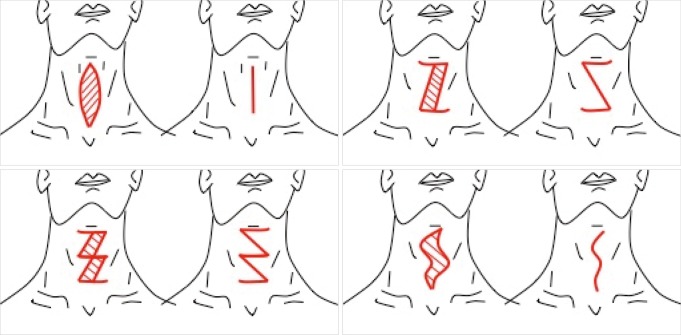
Background: Major problems with cervicoplasty by direct skin excision include the subjective nature of skin markings preoperatively and the confusing array of procedures offered. This technique incorporates curved incisions, resulting in a wave-like scar, which is why the procedure is called a "wave-plasty".
Methods: This prospective study includes 37 patients who underwent wave-plasty procedures from 2004 to 2015. Skin pinching technique was used to mark the anterior neck preoperatively in a reproducible fashion. Intra-operatively, redundant skin was excised, along with excess fat when necessary, and closed to form a wave-shaped scar. Patients were asked to follow up at 1 week, 6 weeks, and 6 months after surgery.
Results: The mean operation time was 70.8 minutes. The majority (81.3%) was satisfied with their progress. On a scale of 1 to 10 (1 being the worst, and 10 being the best), the scars were objectively graded on average 5.5 when viewed from the front and 7.3 when seen from the side 6 months after surgery. Complications consisted of one partial wound dehiscence (2.3%), one incidence of hypertrophic scarring (2.3%), and two cases of under-resection requiring revision (5.4%).
Conclusions: In select patients, surgical rejuvenation of the neck may be obtained through wave-like incisions to remove redundant cervical skin when other options are not available. The technique is reproducible, easily teachable and carries low morbidity and high patient satisfaction in carefully chosen patients.
Keywords: Cervicoplasty; Neck; Rejuvenation.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures






References
-
- Rohrich RJ, Rios JL, Smith PD, et al. Neck rejuvenation revisited. Plast Reconstr Surg. 2006;118:1251–1263. - PubMed
-
- Ramirez OM. Cervicoplasty: nonexcisional anterior approach: a 10-year follow-up. Plast Reconstr Surg. 2003;111:1342–1345. - PubMed
-
- Miller TA. Excision of redundant neck tissue in men with platysma plication and Z-plasty closure. Plast Reconstr Surg. 2005;115:304–313. - PubMed
-
- Chaput B, Grolleau JL, De Bonnecaze G, et al. Anterior medial cervicoplasty. Ann Chir Plast Esthet. 2012;57:612–617. - PubMed
-
- Bitner JB, Friedman O, Farrior RT, et al. Direct submentoplasty for neck rejuvenation. Arch Facial Plast Surg. 2007;9:194–200. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources