

Pregnancy after chemotherapy in male and female survivors of childhood cancer treated between 1970 and 1999: a report from the Childhood Cancer Survivor Study cohort
- PMID: 27020005
- PMCID: PMC4907859
- DOI: 10.1016/S1470-2045(16)00086-3
Pregnancy after chemotherapy in male and female survivors of childhood cancer treated between 1970 and 1999: a report from the Childhood Cancer Survivor Study cohort
Abstract
Background: The effect of many contemporary chemotherapeutic drugs on pregnancy and livebirth is not well established. We aimed to establish the effects of these drugs on pregnancy in male and female survivors of childhood cancer not exposed to pelvic or cranial radiotherapy.
Methods: We used data from a subset of the Childhood Cancer Survivor Study cohort, which followed 5-year survivors of the most common types of childhood cancer who were diagnosed before age 21 years and treated at 27 institutions in the USA and Canada between 1970 and 1999. We extracted doses of 14 alkylating and similar DNA interstrand crosslinking drugs from medical records. We used sex-specific Cox models to establish the independent effects of each drug and the cumulative cyclophosphamide equivalent dose of all drugs in relation to pregnancies and livebirths occurring between ages 15 years and 44 years. We included siblings of survivors as a comparison group.
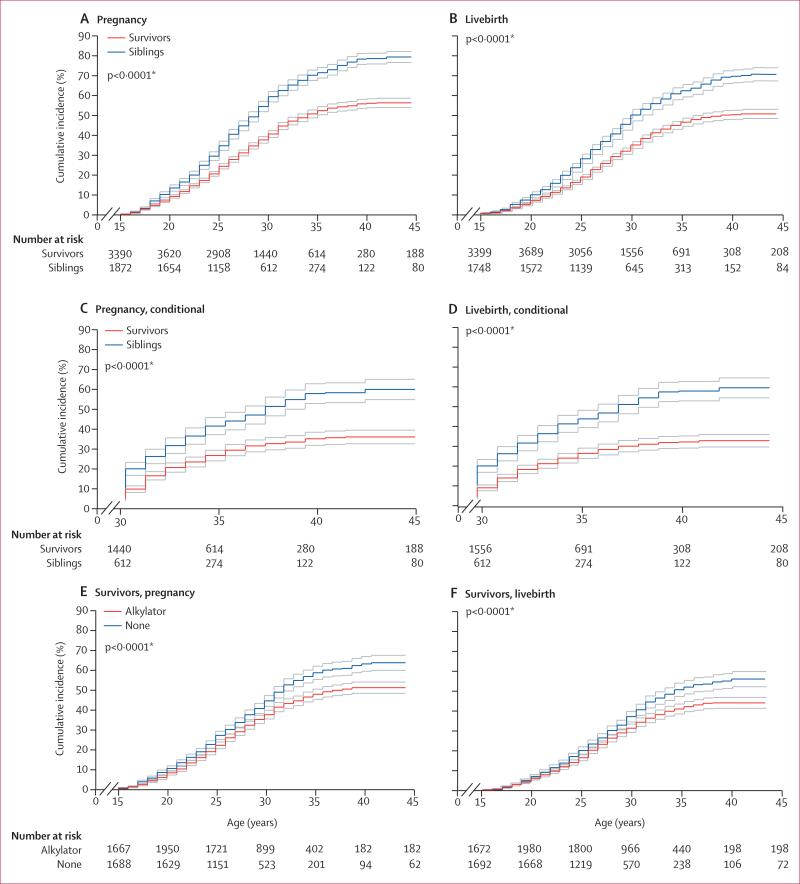
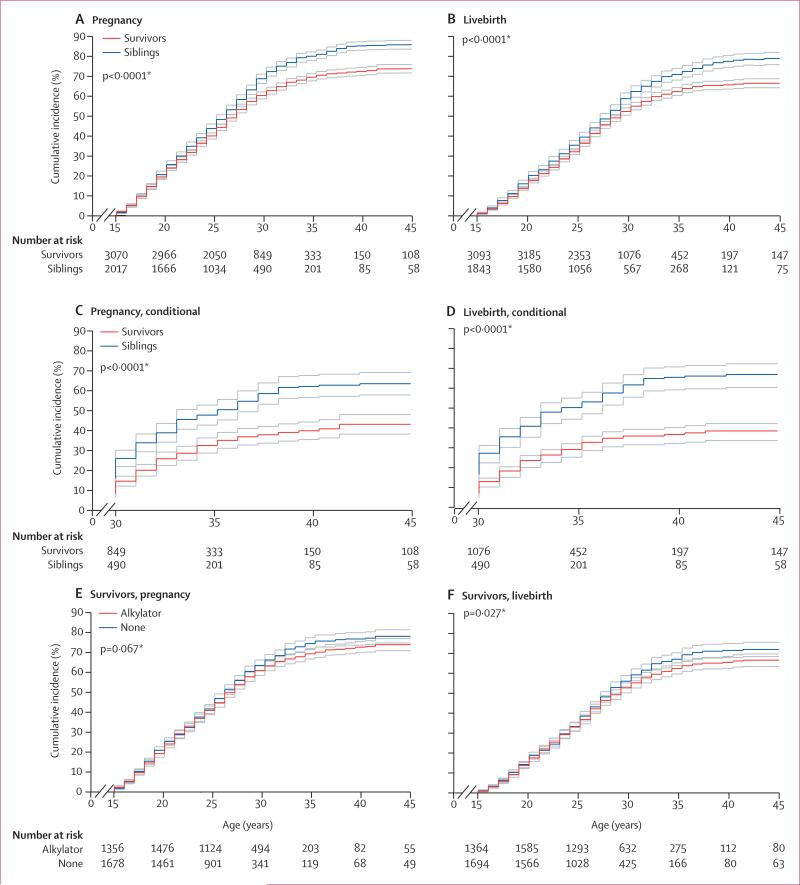
Findings: We included 10 938 survivors and 3949 siblings. After a median follow-up of 8 years (IQR 4-12) from cohort entry or at age 15 years, whichever was later, 4149 (38%) survivors reported having or siring a pregnancy, of whom 3453 (83%) individuals reported at least one livebirth. After a median follow-up of 10 years (IQR 6-15), 2445 (62%) siblings reported having or siring a pregnancy, of whom 2201 (90%) individuals reported at least one livebirth. In multivariable analysis, survivors had a decreased likelihood of siring or having a pregnancy versus siblings (male survivors: hazard ratio [HR] 0·63, 95% CI 0·58-0·68; p<0·0001; female survivors: 0·87, 0·81-0·94; p<0·0001) or of having a livebirth (male survivors: 0·63, 0·58-0·69; p<0·0001; female survivors: 0·82, 0·76-0·89; p<0·0001). In male survivors, reduced likelihood of pregnancy was associated with upper tertile doses of cyclophosphamide (HR 0·60, 95% CI 0·51-0·71; p<0·0001), ifosfamide (0·42, 0·23-0·79; p=0·0069), procarbazine (0·30, 0·20-0·46; p<0·0001) and cisplatin (0·56, 0·39-0·82; p=0·0023). Cyclophosphamide equivalent dose in male survivors was significantly associated with a decreased likelihood of siring a pregnancy (per 5000 mg/m(2) increments: HR 0·82, 95% CI 0·79-0·86; p<0·0001). However, in female survivors, only busulfan (<450 mg/m(2) HR 0·22, 95% CI 0·06-0·79; p=0·020; ≥450 mg/m(2) 0·14, 0·03-0·55; p=0·0051) and doses of lomustine equal to or greater than 411 mg/m(2) (0·41, 0·17-0·98; p=0·046) were significantly associated with reduced pregnancy; cyclophosphamide equivalent dose was associated with risk only at the highest doses in analyses categorised by quartile (upper quartile vs no exposure: HR 0·85, 95% CI 0·74-0·98; p=0·023). Results for livebirth were similar to those for pregnancy.
Interpretation: Greater doses of contemporary alkylating drugs and cisplatin were associated with a decreased likelihood of siring a pregnancy in male survivors of childhood cancer. However, our findings should provide reassurance to most female survivors treated with chemotherapy without radiotherapy to the pelvis or brain, given that chemotherapy-specific effects on pregnancy were generally few. Nevertheless, consideration of fertility preservation before cancer treatment remains important to maximise the reproductive potential of all adolescents newly diagnosed with cancer.
Funding: National Cancer Institute, National Institutes of Health, and the American Lebanese-Syrian Associated Charities.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Female survivors of childhood cancer have good chance of motherhood, study finds.BMJ. 2016 Mar 22;352:i1704. doi: 10.1136/bmj.i1704. BMJ. 2016. PMID: 27009264 No abstract available.
-
Chemotherapy risks to fertility of childhood cancer survivors.Lancet Oncol. 2016 May;17(5):540-1. doi: 10.1016/S1470-2045(16)00116-9. Epub 2016 Mar 22. Lancet Oncol. 2016. PMID: 27020006 No abstract available.
References
-
- Zebrack B, Isaacson S. Psychosocial care of adolescent and young adult patients with cancer and survivors. J Clin Oncol. 2012;30:1221–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
