

KRAS and Combined KRAS/TP53 Mutations in Locally Advanced Rectal Cancer are Independently Associated with Decreased Response to Neoadjuvant Therapy
- PMID: 27020587
- PMCID: PMC5047012
- DOI: 10.1245/s10434-016-5205-4
KRAS and Combined KRAS/TP53 Mutations in Locally Advanced Rectal Cancer are Independently Associated with Decreased Response to Neoadjuvant Therapy
Abstract
Background: The response of rectal cancers to neoadjuvant chemoradiation (CRT) is variable, but tools to predict response remain lacking. We evaluated whether KRAS and TP53 mutations are associated with pathologic complete response (pCR) and lymph node metastasis after adjusting for neoadjuvant regimen.
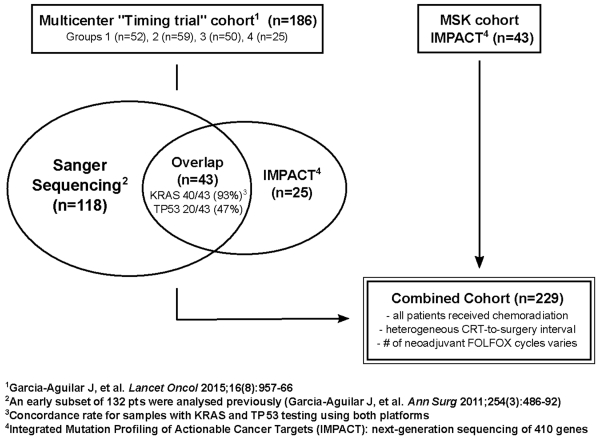
Methods: Retrospective analysis of 229 pretreatment biopsies from patients with stage II/III rectal cancer was performed. All patients received CRT. Patients received 0-8 cycles of FOLFOX either before or after CRT, but prior to surgical excision. A subset was analyzed to assess concordance between mutation calls by Sanger Sequencing and a next-generation assay.
Results: A total of 96 tumors (42 %) had KRAS mutation, 150 had TP53 mutation (66 %), and 59 (26 %) had both. Following neoadjuvant therapy, 59 patients (26 %) achieved pCR. Of 133 KRAS wild-type tumors, 45 (34 %) had pCR, compared with 14 of 96 (15 %) KRAS mutant tumors (p = .001). KRAS mutation remained independently associated with a lower pCR rate on multivariable analysis after adjusting for clinical stage, CRT-to-surgery interval and cycles of FOLFOX (OR 0.34; 95 % CI 0.17-0.66, p < .01). Of 29 patients with KRAS G12V or G13D, only 2 (7 %) achieved pCR. Tumors with both KRAS and TP53 mutation were associated with lymph node metastasis. The concordance between platforms was high for KRAS (40 of 43, 93 %).
Conclusions: KRAS mutation is independently associated with a lower pCR rate in locally advanced rectal cancer after adjusting for variations in neoadjuvant regimen. Genomic data can potentially be used to select patients for "watch and wait" strategies.
References
-
- Smith JD, Ruby JA, Goodman KA, et al. Nonoperative management of rectal cancer with complete clinical response after neoadjuvant therapy. Ann Surg. 2012;256(6):965–972. doi:10.1097/SLA.0b013e3182759f1c. - PubMed
-
- Guillem JG, Chessin DB, Shia J, et al. Clinical examination following preoperative chemoradiation for rectal cancer is not a reliable surrogate end point. J Clin Oncol. 2005;23(15):3475–3479. doi:10.1200/JCO.2005.06.114. - PubMed
-
- Radovanovic Z, Breberina M, Petrovic T, Golubovic A, Radovanovic D. Accuracy of endorectal ultrasonography in staging locally advanced rectal cancer after preoperative chemoradiation. Surg Endosc. 2008;22(11):2412–2415. doi:10.1007/s00464-008-0037-3. - PubMed
-
- Huh JW, Park YA, Jung EJ, Lee KY, Sohn S-K. Accuracy of endorectal ultrasonography and computed tomography for restaging rectal cancer after preoperative chemoradiation. J Am Coll Surg. 2008;207(1):7–12. doi:10.1016/j.jamcollsurg.2008.01.002. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
