

The Role of Complement Inhibition in Thrombotic Angiopathies and Antiphospholipid Syndrome
- PMID: 27020721
- PMCID: PMC4805354
- DOI: 10.4274/tjh.2015.0197
The Role of Complement Inhibition in Thrombotic Angiopathies and Antiphospholipid Syndrome
Abstract
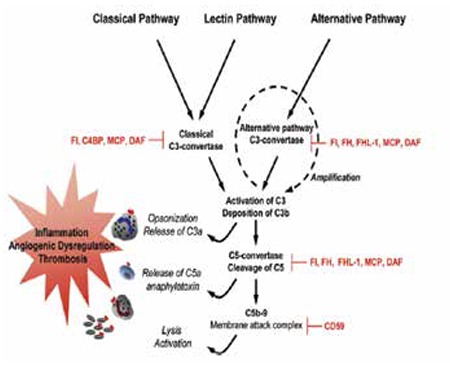
Antiphospholipid syndrome (APS) is characterized by thrombosis (arterial, venous, small vessel) and/or pregnancy morbidity occurring in patients with persistently positive antiphospholipid antibodies (aPL). Catastrophic APS is the most severe form of the disease, characterized by multiple organ thromboses occurring in a short period and commonly associated with thrombotic microangiopathy (TMA). Similar to patients with complement regulatory gene mutations developing TMA, increased complement activation on endothelial cells plays a role in hypercoagulability in aPL-positive patients. In mouse models of APS, activation of the complement is required and interaction of complement (C) 5a with its receptor C5aR leads to aPL-induced inflammation, placental insufficiency, and thrombosis. Anti-C5 antibody and C5aR antagonist peptides prevent aPL-mediated pregnancy loss and thrombosis in these experimental models. Clinical studies of anti-C5 monoclonal antibody in aPL-positive patients are limited to a small number of case reports. Ongoing and future clinical studies of complement inhibitors will help determine the role of complement inhibition in the management of aPL-positive patients.
Antifosfolipid sendromu (APS), ısrarcı antifosfolipid antikor (aPL) pozitifliği olan hastalarda görülen tromboz (arteriyel, venöz, küçük damar) ve/veya gebelik ile ilişkili morbidite ile karakterizedir. Hastalığın en şiddetli formu olan katastrofik APS, kısa süre içerisinde gelişen çoklu organ trombozları ile karakterizedir ve sıklıkla trombotik mikroanjiyopati (TMA) ile ilişkilidir. TMA geliştiren kompleman düzenleyici gen mutasyonları bulunan hastalarla benzer olarak, aPL-pozitif hastalardaki hiperkoagülopatide, endotel hücrelerinde artmış kompleman aktivasyonunun rolü vardır. APS’nin fare modellerinde, kompleman aktivasyonunun olması zorunludur ve kompleman (C) 5a ile reseptörü C5aR’nin etkileşmesi aPL-ile uyarılmış yangı, plasenta yetmezliği ve tromboza neden olur. Anti-C5 antikoru ve C5aR antagonisti olan peptidler bu deneysel modellerde, aPL-aracılı gebelik kaybı ve trombozu önler. aPL-pozitif hastalarda anti-C5 monoklonal antikorun klinik kullanımı az sayıdaki olgu sunumları ile sınırlıdır. Halen devam etmekte olan ve gelecekte yapılacak klinik çalışmalar, aPL-pozitif hastaların yönetiminde kompleman inhibitörlerinin rolünü belirlemede yardımcı olacaktır.
Conflict of interest statement
Conflict of Interest: Doruk Erkan and Jane Salmon: Alexion (Clinical Trial Investigator, Advisory Board)
Figures
Similar articles
-
Complement in the Pathophysiology of the Antiphospholipid Syndrome.Front Immunol. 2019 Mar 14;10:449. doi: 10.3389/fimmu.2019.00449. eCollection 2019. Front Immunol. 2019. PMID: 30923524 Free PMC article. Review.
-
Complement and the antiphospholipid syndrome.Curr Opin Hematol. 2011 Sep;18(5):361-5. doi: 10.1097/MOH.0b013e3283497f3e. Curr Opin Hematol. 2011. PMID: 21730831 Review.
-
Antiphospholipid antibody syndrome.Obstet Gynecol Clin North Am. 2014 Mar;41(1):113-32. doi: 10.1016/j.ogc.2013.10.004. Obstet Gynecol Clin North Am. 2014. PMID: 24491987 Review.
-
Secondary thrombotic microangiopathy in systemic lupus erythematosus and antiphospholipid syndrome, the role of complement and use of eculizumab: Case series and review of literature.Semin Arthritis Rheum. 2019 Aug;49(1):74-83. doi: 10.1016/j.semarthrit.2018.11.005. Epub 2018 Dec 4. Semin Arthritis Rheum. 2019. PMID: 30598332 Review.
-
The role of complement in the antiphospholipid syndrome: a novel mechanism for pregnancy morbidity.Semin Arthritis Rheum. 2012 Aug;42(1):66-9. doi: 10.1016/j.semarthrit.2012.01.001. Epub 2012 Mar 8. Semin Arthritis Rheum. 2012. PMID: 22405029 Review.
Cited by
-
Complement C5 but not C3 is expendable for tissue factor activation by cofactor-independent antiphospholipid antibodies.Blood Adv. 2018 May 8;2(9):979-986. doi: 10.1182/bloodadvances.2018017095. Blood Adv. 2018. PMID: 29716893 Free PMC article.
-
Effect of Tumor Red Blood Cell Immunity and Tumor Cell Cycle in Mice Bearing Solid Liver Cancer with Intelligent Cancer Zhongning Therapeutic Apparatus.J Healthc Eng. 2021 Jun 4;2021:3329800. doi: 10.1155/2021/3329800. eCollection 2021. J Healthc Eng. 2021. Retraction in: J Healthc Eng. 2023 Jan 20;2023:9794260. doi: 10.1155/2023/9794260. PMID: 34194680 Free PMC article. Retracted.
-
Complement in Secondary Thrombotic Microangiopathy.Kidney Int Rep. 2021 Jan;6(1):11-23. doi: 10.1016/j.ekir.2020.10.009. Epub 2020 Oct 21. Kidney Int Rep. 2021. PMID: 33102952 Free PMC article. Review.
-
Eculizumab in refractory catastrophic antiphospholipid syndrome: a case report and systematic review of the literature.Clin Exp Med. 2019 Aug;19(3):281-288. doi: 10.1007/s10238-019-00565-8. Epub 2019 Jun 18. Clin Exp Med. 2019. PMID: 31214910
-
Pathogenic Role of Complement in Antiphospholipid Syndrome and Therapeutic Implications.Front Immunol. 2018 Jun 19;9:1388. doi: 10.3389/fimmu.2018.01388. eCollection 2018. Front Immunol. 2018. PMID: 29971066 Free PMC article.
References
-
- Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, Derksen RH, DE Groot PG, Koike T, Meroni PL, Reber G, Shoenfeld Y, Tincani A, Vlachoyiannopoulos PG, Krilis SA. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost. 2006;4:295–306. - PubMed
-
- Girardi G, Redecha P, Salmon JE. Heparin prevents antiphospholipid antibody-induced fetal loss by inhibiting complement activation. Nat Med. 2004;10:1222–1226. - PubMed
-
- Hillmen P, Young NS, Schubert J, Brodsky RA, Socié G, Muus P, Röth A, Szer J, Elebute MO, Nakamura R, Browne P, Risitano AM, Hill A, Schrezenmeier H, Fu CL, Maciejewski J, Rollins SA, Mojcik CF, Rother RP, Luzzatto L. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355:1233–1243. - PubMed
-
- Legendre CM, Licht C, Muus P, Greenbaum LA, Babu S, Bedrosian C, Bingham C, Cohen DJ, Delmas Y, Douglas K, Eitner F, Feldkamp T, Fouque D, Furman RR, Gaber O, Herthelius M, Hourmant M, Karpman D, Lebranchu Y, Mariat C, Menne J, Moulin B, Nürnberger J, Ogawa M, Remuzzi G, Richard T, Sberro-Soussan R, Severino B, Sheerin NS, Trivelli A, Zimmerhackl LB, Goodship T, Loirat C. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368:2169–2181. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous